Playlist
Show Playlist
Hide Playlist
Diagnosis: Chest X-ray and Ct Scan – Lung Disease


-
Slides 06 Respiratory Medicine Basics Brown.pdf
-
Download Lecture Overview
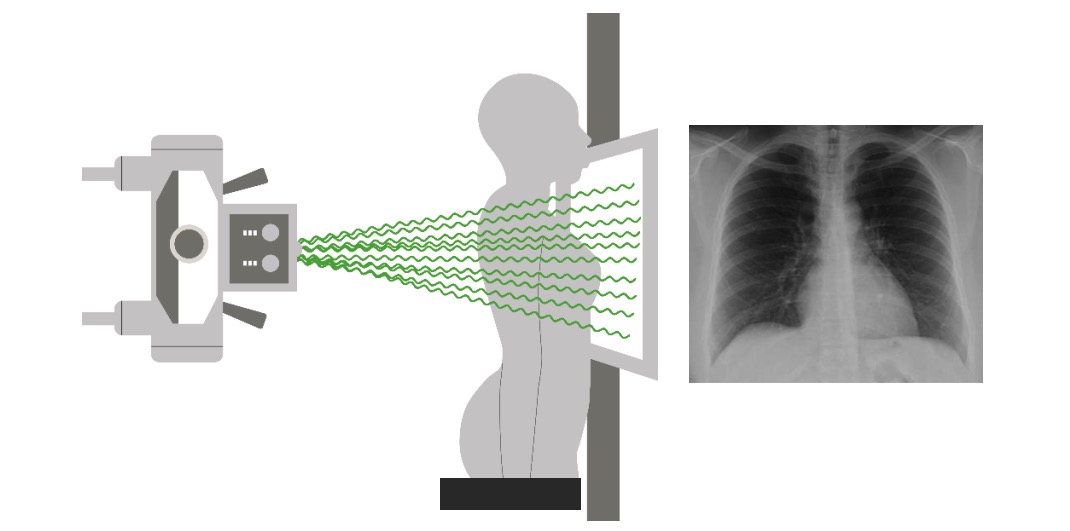
00:01 The chest x-ray remains the main investigation that we use for patients presenting with lung disease. And it’s used basically to screen to make sure there are no major abnormalities of the lung. 00:10 This is a normal chest x-ray with each structures identified. I’m not going to go through that in turn but the important point to note here is that the lungs look black. And that’s because they’re full of air. And most problems that occur that you can pick up on a chest x-ray will cause either liquid or solid material to occur in an area where there should be blackness due to the lung. 00:34 So you can see this in this example here. There’s a left pleural effusion. That’s fluid in the pleural space. And the bottom of the left lung is now all white as a consequence of that fluid showing up on the x-ray. 00:47 This patient’s got an interstitial lung disease with infiltration of the upper lobes of their lung with sarcoid tissue. And that shows up as not very distinct but clearly present areas of white infiltrations in both upper lobes. 01:00 And this patient has a TB. And that’s affecting the top of the right lung and, again, you can see there’s some white shadowing there. The main exception to the white shadowing situation is that, if you have a pneumothorax or a large cyst in the lung full of air, that shows up as black tissue instead of white. But largely what we’re looking for are areas of increased white or grey shadowing in the lung. 01:26 Now the CT scan is a fantastic test for providing three-dimensional lung anatomy information. 01:31 It provides multiple slices through the lung and allows you to assess in very great detail the parenchymal structure, the mediastinal structure, the bones and the joints, depending on which setting you use. In fact, if you inject contrast into the patient and time it correctly, you can also delineate the pulmonary arteries very clearly and identify pulmonary emboli. 01:51 The problem with the CT scan is that it does require quite a substantial radiation dose compared to a chest x-ray. It takes more time. It requires somebody to be able to hold their breath and not be claustrophobic. And many patients find that very difficult. And the contrast that is used in some CT scans can have nephrotoxic problems. It can cause or precipitate renal failure, for example, and it can cause exacerbations of asthma in susceptible patients. 02:19 The CT scan though is now an established method of assessing lung diseases of a specific type. 02:24 So, for example, if you suspect somebody has a lung tumour, then the CT scan is absolutely important. If you suspect they have interstitial lung disease, again the CT scan is vital. 02:34 Pulmonary emboli: the main method of identifying those nowadays is a CT pulmonary angiogram. 02:38 And there’s various other diseases that are best detected by a CT scan where the chest x-ray is either insensitive or does not give accurate enough information to tell you exactly what’s going on, such as bronchiectasis or the presence of emphysema. And then if you’re looking for small lesions that might be causing haemoptysis, or mediastinal abnormalities which are mainly hidden here in the chest x-ray and are difficult to see, then the CT scan is very helpful. 03:02 So just to give an example, this is somebody who’s had a bone-marrow transplantation, they’ve got a fever and the x-ray doesn’t really show much. But if you look at the top of the left lung, there’s a little bit of shadowing there compared to the right lung. 03:16 Now, if you do a CT scan, it actually becomes very obvious that what’s happening there is there is a 3-4 cm mass at the top of the left lung. And this has the characteristics suggestive of a fungal infection. And that allows you to treat this patient without any further investigation if you wanted to. It just shows the added value you get from a three-dimensional additional image compared to just the plain chest x-ray. This green line indicates the level of the scan. 03:43 So there are other x-ray modalities that we use in lung disease. Ultrasound for example is very useful in assessing pleural disease – and I’m not going to discuss that any more. That’s a picture of an ultrasound showing a pleural effusion where you can clearly see the fluid lying between the chest wall and the lung. 03:56 Pulmonary angiogram: that’s a method where you inject contrast directly into the pulmonary arteries to visualise them in detail. This is somebody who has actually clogged off their left pulmonary artery with an embolus. And you can see the contrast going through the arteries on the right-hand side but actually very little contrast is visible on the left-hand side. 04:14 And the MRI scan actually is not terribly useful for lung disease but is useful for the areas around the lung: the chest wall and the vertebrae. And this is an MRI scan showing somebody with spinal tuberculosis and you can see destruction of the vertebra present where the arrows are indicating. 04:30 We also use radionucleotide scan. This is where you inject a radionucleotide tracer and that will go to specific types of tissue. So, for example, there’s a tracer which we use for bone scans to identify whether there are any lesions in the bone. And there’s a ventilation [Inaudible 0:32:56] use for ventilation/perfusion scans. This is one of the older methods for identifying pulmonary emboli that is used less and less nowadays where you inhale a radioactive tracer and inject a radioactive tracer and you match where the distribution is of those two. And a PE will show up when somebody has an area which is ventilated but not perfused. 05:04 And actually the most important of the radionucleotide scans nowadays is what we call a PET scan using radio-labelled glucose. Now that’s very important because that goes to areas of active cell metabolism. So it goes where there’s malignancies and it goes where there’s an infection and it’s a very useful test for investigating patients with lung cancer to assess where the cancer may be – may have spread to. So it’s a staging test for lung cancer. And we use it in other circumstances when monitoring patients with some types of infections and active inflammatory lung diseases. 05:41 So the final resort normally with every type of investigation is to try and obtain a histological sample. And actually for the majority of lung diseases that’s not necessary. However, for some lung diseases it’s vital. So, for example, a suspected cancer is absolutely essential to get histological confirmation. The same is true for somebody with chronic sarcoidosis and the same is true for patients with some types of infection and other lung inflammatory conditions. 06:13 And there are actually many different methods for obtaining lung tissue by biopsy. The commonest are CT- or ultrasound-guided biopsies of the pleura, CT-guided biopsies of the lung, bronchoscopic biopsies that we’ve discussed already, which can be endobronchial, transbronchial or the endobronchial ultrasound biopsies of the lymph nodes. And then, in the last resort, you can do surgical biopsies and this could be of the mediastinal nodes or they could be of the lung tissue. And those are normally done by video-assisted thoracoscopic surgical techniques but they do require a general anaesthetic, an operation and probably being in hospital for 3 to 4 days, which is quite a heavy problem for somebody who’s having a diagnostic test as supposed to a surgery for a curative reason.
About the Lecture
The lecture Diagnosis: Chest X-ray and Ct Scan – Lung Disease by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Introduction to the Respiratory System.
Included Quiz Questions
Which of the following is NOT a common indication for bronchoscopy?
- Community acquired pneumonia
- Hemoptysis
- Lobar collapse
- Suspected sarcoidosis
All of the following are downsides of CT scans, except...?
- ...they have overall lower sensitivity than chest X-rays.
- ...they require higher doses of radiation.
- ...they require breath-holding.
- ...the IV contrast may be nephrotoxic.
- ...they may provokde claustrophobia in some patients.
Which of the following is NOT an indication for a chest CT scan?
- Asthma
- Lung masses (e.g. tumors, cavitating lesions)
- Pulmonary embolism
- Hemoptysis
- Suspected mediastinal abnormalities
Author of lecture Diagnosis: Chest X-ray and Ct Scan – Lung Disease

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good overview of the different scans used to examine lungs and specific uses for each.
