Playlist
Show Playlist
Hide Playlist
Wrist and Hand

-
Slides Osteopathic Considerations of the Upper Extremity.pdf
-
Download Lecture Overview
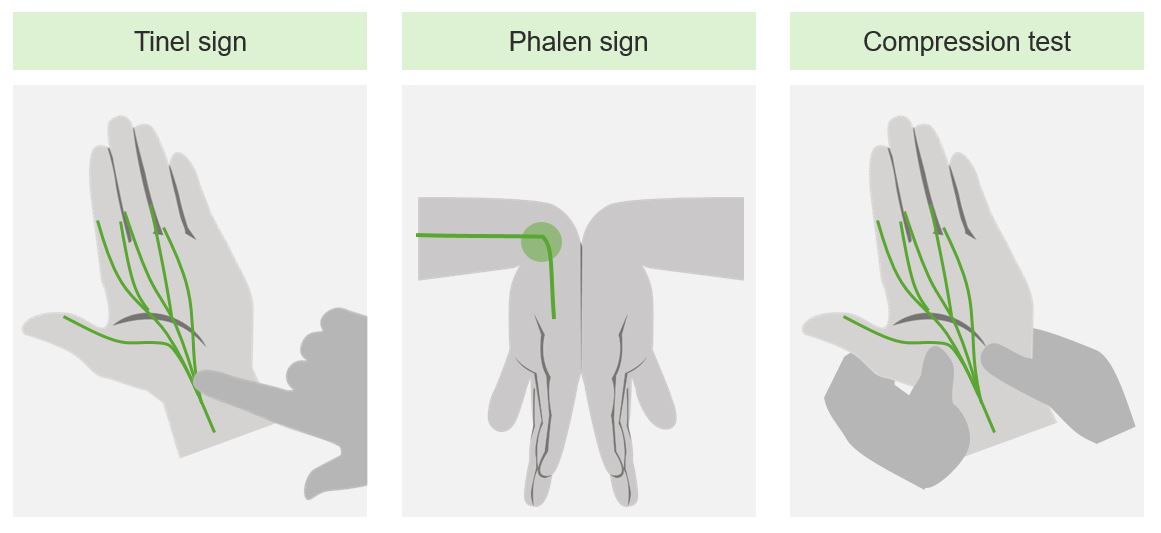
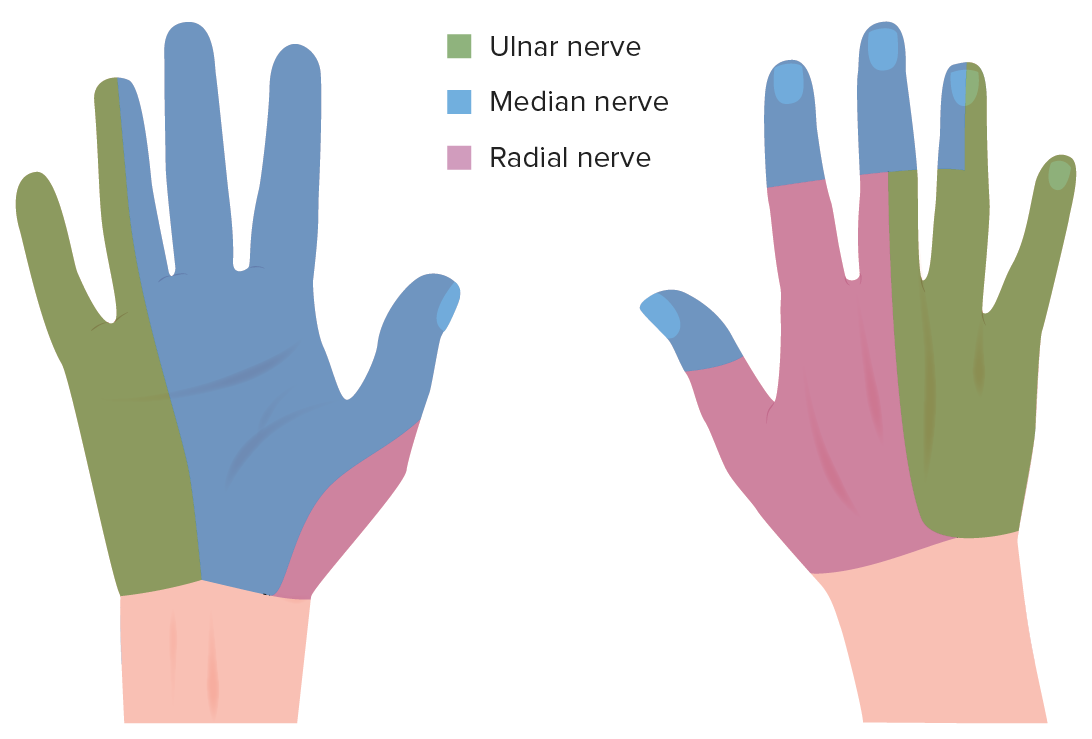
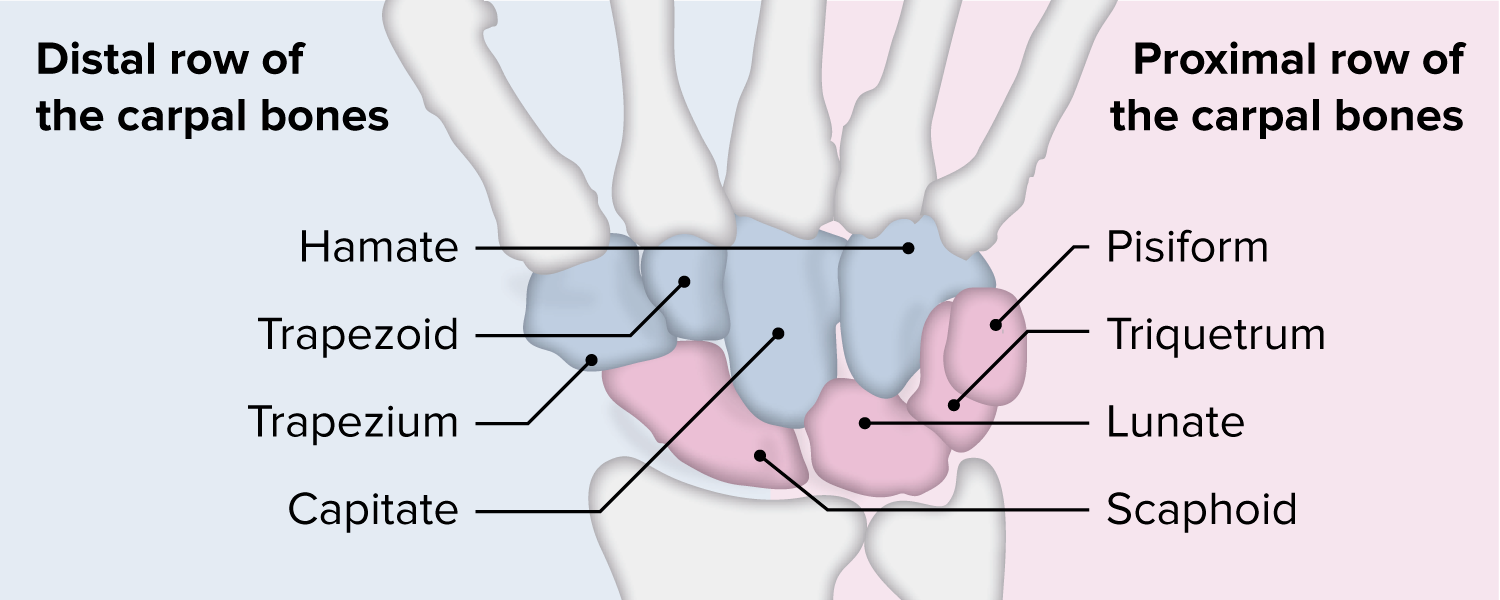
00:01 With wrist and hand anatomy, the hand is a closed space. 00:06 Knowing the bones and knowing the muscles are important, being able to differentiate the carpals and the metacarpals from the phalanges is your first step. 00:15 So you deal with the carpal bones on the wrist and the metacarpal bones which are the fingers hidden by the hand and the phalanges of the fingers. 00:23 Learning the ligaments is also gonna be critical to being able to talk with the hand surgeon or somebody who may be able to help you with issues related to the hand. 00:33 The nerve distribution is very clear and can tell you where you may have impingements everywhere. 00:38 So the hand is a good harbinger of illness elsewhere and knowing the median nerve disrtibution and ulnar nerve distribution will help you separate out those pathologies. 00:50 The range of motion of the hand is that you can have extension to 70, flexion to 80. 00:55 You'll have radial deviation up to 20 and ulnar deviation to 30 degrees. 01:00 and you have finger adduction and abduction as well. 01:04 So complicated movement, lots of movement and lots of trauma to the hand as well. 01:10 If somebody has decreased range of motion, it could be secondary to spasm, it could be secondary to tendon or ligament issues and doing the test to figure out which it is, is important because again, damage to the hand can occur quickly and needs to be taken seriously. 01:29 We do a lot of motion testing of the hand to see if there's a loss of hand or whether people just have overuse injuries which are also very common with spasm and pain in the hand. 01:41 It is not unusual to use muscle energy techniques to help with muscle pain and the hand pain as a way of helping. 01:50 One of the more chronic issues we see a lot is De Quervain's tenosynovitis which is a contracture of the ligaments and a loss of use of the hand because of the contracture. 02:03 It also causes instability of some of the bones and the wrist area. 02:07 So it's something that needs to be paid attention to. 02:10 The physiology of De Quervain's or inflammation of the extensor pollicis brevis and the abductor pollicis longus tendons which can contract and can stay contracted and you can have a loss of some of the motion. 02:24 The test is called Finkelstein's test where you put the thumb inside the hand and squeeze. 02:29 Severe pain is a positive test. 02:32 The osteopathic treatment of De Quervain's is to increase the radial deviation, helping with the motion by restoring motion either by muscle energy or counterstrain. 02:45 Other injuries to worry about are ligamentous injuries that could affect the scapholunate stability or perilunate stability. 02:53 Ligamentous strain or rupture can cause a gap in the area and this thing should be watched for and monitored for. 03:01 So you wanna do a good hand exam and again, knowing the anatomy and knowing where you're testing them is going to be a big help. 03:09 We're gonna go through Watson's test, there'll be a separate video on that, so you'll have a short video to be able to test for ligamentous injury of the hand. 03:18 The test for perilunate instability is called the Shuck test and again, we'll do a separate video looking at the Shuck test for hand instability and finger instability. 03:28 Severe pain is going to indicate this instability and needs to be looked up further. 03:34 We are gonna have a separate talk on carpal tunnel syndrome and we'll talk a little bit about injury to the ulnar nerve distal posterior interosseous nerve syndrome and a vascular compromise to the hand. 03:46 Carpal tunnel is a very common condition and it's letting people come to for treatment for. 03:52 Because we've got good treatments and interventions that will help. 03:56 The physiology of carpal tunnel syndrome is this is an entrapment syndrome. 04:00 It's a neuropathy of the median nerve as it passess through the carpal tunnel. 04:05 And the flexor tendons tend to get taught, limit motion and tend to spasm. 04:12 If you can reproduce pain with the Tinel's test, just tapping on the carpal tunnel and you get shooting pain to the fingers, that's a positive Tinel's sign and can be indicative of carpal tunnel syndrome. 04:26 The osteopathic management is stretching and relief of symptoms. 04:32 And what I do is I put my hand between the 4th digit and the 1st digit, stretch out the hand, pull the carpal tunnel and help induce increased motion that way. 04:43 You will keep the hand dosriflexed at the wrist and splaying the fingers and stretching. 04:50 and we'll have a separate video on that as well. 04:53 Osteopathic management focuses on the carpal bones and the carpal tunnel. 04:58 Some people do do HVLA, it is an easier, quicker way of doing it but with the pain, some patients are uncomfortable with it. 05:06 and what you do is you get a good grip of the carpal bones and when you have a restriction, you find the area where the restriction is and then work through that restriction. 05:17 It helps to have the hand dorsiflexed until you engage the barrier. 05:21 And then employ immobilization with a thrust moving towards the wrist, to the floor with the hand down. 05:28 The palmar flexor barrier can be engaged as well, if you wanna do a high velocity, low amplitude thrust technique, to treat a carpal tunnel syndrome. 05:37 We can treat it in other ways as well. 05:40 If you wanna treat it with joint mobilization, you will grasp the hand and it can be done either pronated or supinated, find the area where the restriction is and once you've engaged the restriction, work through the barrier. 05:56 You can apply an upward force if you got the hand supinated in order to engage and treat the carpal tunnel syndrome. 06:03 There will be a more thorough discussion of carpal tunnel syndrome in another lecture. 06:07 If you have injury to the ulnar nerve through Guyon's canal, that's a compression of the ulnar nerve as it passess between the pisiform and the hook of hamate. 06:17 Also very serious, it happens with trauma and it is something that needs to be treated. 06:22 The Tinel's test will also tell you if there is an impingement of this nerve. 06:29 Positive test is when you have the radiation of pain down the nerve root. 06:36 Management is activity modification and splinting beacause this is an overuse injury and at times, steroid or corticosteroid injections will help. 06:45 From the osteopathic perspective, we'll do some myofascial release to help ease the symptoms and help relieve the pain of Guyon's canal syndrome and the ulnar nerve impingement. 06:56 For the distal posterior interosseous nerve syndrome, the physiology is one of entrapment of the posterior interosseous nerve and it can cause finger weakness and difficulties with wrist extension with preserved sensation. 07:12 We will treat this as other impingement syndromes with positioning and bracing as well. 07:18 From Osteopathic perspective, we can use myofascial release to help ease up with the symptoms and help make people feel better. 07:26 So if you grasp the patient's distal forearm and hold them by the thumbs, that's one way to help stretching and the myofascial release. 07:36 You'll do some effleurage, you'll do some massage and free up the tissues that way. 07:43 And the last nerve vascular issue is gonna be vascular compromise. 07:48 Again, this could be a medical emergency and needs immediate intervention. 07:52 If there's a change in the vasculature supply in the hand, there'll be ischemic pain and severe pain immediately. 08:00 We do the Allen test to see if you have a good pulse in both the radial and ulnar arteries And what you do is you have the patient open and close the fist and you occlude the radial and ulnar arteries, and then you release one at a time, making sure that the hand fills with blood, that you have increased perfussion after relaxing or relieving each the radial and ulnar vessels. 08:26 If it stays pale when you release the artery, it's a sign that there might not be good perfussion and you may need further intervention. 08:37 So if the palm does not flush, that's a positive Allen's test. 08:42 Those are the probs of the upper extremity. 08:44 Thank you for listening.
About the Lecture
The lecture Wrist and Hand by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by Region. It contains the following chapters:
- Wrist and Hand Anatomy
- Wrist and Hand Pathologies
- Wrist and Hand Neurovasculature
Included Quiz Questions
Which of the following upper extremity physical examination tests is used in the evaluation of De Quervain's tenosynovitis?
- Finkelstein's test
- Phalen's test
- Tinel's sign
- Cozen's test
- Yergason's test
A 32-year-old writer presents to the clinic with numbness in the thumb, index, and middle finger of her right hand. She notes that the symptoms began recently when she started to write her second book. On osteopathic structural examination, you note that tapping the area of the median nerve at the volar right wrist reproduces numbness and tingling sensation in the thumb, index, and middle finger of her right hand. What is the most likely diagnosis?
- Carpal tunnel syndrome
- Guyon's canal syndrome
- Cubital tunnel syndrome
- Tarsal tunnel syndrome
- De Quervain's tenosynovitis
Which of the following special tests is used in the assessment of the vascular integrity or vascular compromise in the hand?
- Allen's test
- Adson's test
- Empty can test
- Spurling's test
- Tinel's sign
Author of lecture Wrist and Hand

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
