Playlist
Show Playlist
Hide Playlist
Whipple Disease

-
Slides GIP Whipple Disease.pdf
-
Download Lecture Overview
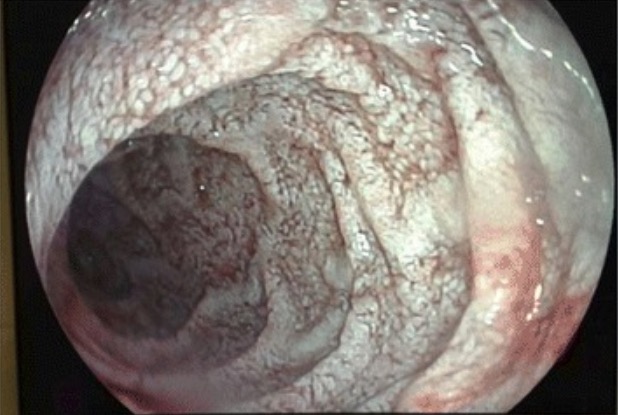
00:01 Welcome. 00:02 With this talk, we're going to cover Whipple's Disease. 00:05 This is not exactly a public health menace, and you may never see a case in your entire career. 00:11 But when you do, you won't forget it. 00:15 So Whipple's disease is a relatively rare malabsorption syndrome that does have systemic manifestations including things involving the central nervous system, a heart and the musculoskeletal system. 00:28 And it's caused specifically by one bacteria, the bacterium Tropheryma whipplei. 00:33 And you're probably thinking to yourself, "Why is there a bearskin rug here?" We'll see why that is in a moment. 00:41 But I'll tell you that the characteristic lesions in the GI tract have been likened to the fur on a bearskin rug. 00:50 At least you won't forget it. 00:53 The epidemiology. 00:54 There is a worldwide distribution, the bacterium Tropheryma whipplei is present throughout the world. 01:01 It is more commonly affecting older males. 01:06 And it is specifically associated with the HLA-B27 haplotype. 01:11 In fact, it's not because it's more of an autoimmune disease, but because you don't specifically elicit a strong immune response to the bacterium. 01:20 And that's why you get the disease. 01:22 The mean age of symptom onset is in the latter half of life over the age of 50. 01:28 There are rare cases that will happen in the pediatric population. 01:31 The pathophysiology of this disease. 01:33 So again, the causal agent is Tropheryma whipplei, I probably ought to remember that, it's one of the bugs that you should remember. 01:41 And it's a host. 01:42 It's not an immunodeficiency, but it's a hole in the immune repertoire. 01:48 And you will have diminished helper type 1, and increased helper type 2 responses to this particular bacteria. 01:56 For the vast majority of the population, you have a very robust Th1 or helper type 1 response and that typically will eliminate the microorganism. 02:06 If you don't have that good robust response, then you will have reduced macrophage activation. 02:11 And what happens is macrophages will ingest, they will phagocytose the organism, but they don't, they don't kill it. 02:19 And so the organism very happily proliferates within the macrophage that has eaten them. 02:24 And with time, you will get an overwhelming infection. 02:30 When this happens, you get lots and lots and lots of very overstuffed macrophages within the lamina propria. 02:37 And that leads to increased transit distance and therefore poor absorption. 02:42 And I'll show you what that looks like on this slide here. 02:46 This is a Periodic acid-Schiff or a PAS stained slide that highlights glycoproteins the very dark intense pink material is glycoprotein. 02:58 And in this particular case that means bacterium the Tropheryma whipplei. 03:03 The taller columnar blue looking cells all the way around are the epithelium. 03:08 So the epithelium is intact, we have normal villi length, we have normal crypt depth. 03:15 But what we have is expanded lamina propria. 03:18 So the epithelium lining the lamina propria is absorbing just fine. 03:25 But the organisms are by expanding the lamina propria are increasing the transit distance, the diffusion distance for things that get absorbed and we are overall getting less material into the bloodstream and into lymphatics. 03:41 And along the way, the bacteria are also happily metabolizing everything. 03:46 What does this look like on endoscopy? So here's our bearskin rug. 03:49 Underneath the green patches, you see areas where there's very distended villi. 03:55 It's someone maybe with a lot of caffeine on board. 03:59 I thought, I think that looks like a bearskin rug, whatever. 04:03 But that's a very characteristic appearance. 04:06 It's not just in the GI tract, any organ, which is every organ that has macrophages can potentially have manifestations related to the accumulation of the bacterium. 04:17 So the intestinal epithelium is a significant target. 04:22 And that's why it's represented here in GI pathophysiology. 04:25 But it can happen in capillary and lymphatic endothelium throughout the body, and then in the liver, the brain, kidneys, everywhere there's a macrophage and that's everywhere. 04:35 You can get an accumulation, you can get secondary manifestations. 04:39 The clinical presentation. 04:41 So the GI manifestations are all about the malabsorption. 04:44 You're gonna have diarrhea because you're going to have osmotic material that isn't being appropriately absorbed, and the bacteria, well, that osmotic force is going to pull fluid into the GI tract and you'll have diarrhea. 04:58 You will also not absorb fats appropriately. 05:00 So you'll have foul smelling floating stool. 05:05 There will be weight loss because there's malnutrition. 05:07 There'll be abdominal pain because the bacteria are happily fermenting all of those metabolites that aren't being absorbed. 05:14 And they will cause gas formation which will distend the bowel which causes abdominal pain. 05:21 There is also an inflammatory response. 05:24 It's not just the macrophages that are present within the lamina propria. 05:27 But we may also see macrophages that are in the draining nodes also be expanded. 05:33 So there'll be lymphadenopathy, kind of throughout the GI tract. 05:37 Peripheral edema happens as a result of malnutrition. 05:40 You're not making the appropriate amounts of albumin so your oncotic pressure is diminished. 05:46 Outside of the GI tract, you can have cardiac manifestations. 05:49 So you can have endocarditis involving the valves, myocarditis involving the myocardium, pericarditis involving the lining around the heart. 05:57 And it can eventually progress to congestive heart failure. 06:02 In the CNS in the brain, you can have seizures, delirium, you can sleep all the time, you can have abnormal walking, you may have abnormal muscle jerking or clonus. 06:12 And arthralgias with involvement of the vasculature within the joints. 06:19 How do we make the diagnosis? Well, sometimes this is one of those entities that patients, the poor patient who has this, they go and see multiple different doctors, before someone thinks to himself, "Could this be Whipple's disease?" Once you get that notion that all these funny manifestations and malabsorption, diarrhea, etc. 06:42 Once you think, "Gosh, maybe this is Whipple's?" This is a very rare patient, then you will do endoscopy. 06:48 And endoscopy on small bowel biopsy, makes your diagnosis. 06:52 So hurray, again, for the pathologist. 06:57 Management. 06:59 Basically, it's a bug. 07:00 It is a bacterium. 07:01 So it's going to be responsive to antibiotics which is fortunate. 07:04 If you make the diagnosis, you can cure your patient. 07:07 I don't think you need to memorize which antibiotics work. 07:10 Just think, "Oh, it's bacteria, we ought to be able to treat this." It is important to realize that if there is central nervous system involvement, you have a blood brain barrier that normally blocks a lot of antibiotics. 07:22 So you need to select those that will penetrate that particular barrier. 07:26 Snd with that, a relatively rare entity, kind of an interesting discussion and hopefully you'll never forget the bearskin rug.
About the Lecture
The lecture Whipple Disease by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
Which bacterium is associated with Whipple disease?
- Tropheryma whipplei
- Yersinia enterocolitica
- Bacillus cereus
- Escherichia coli
- Streptococcus pneumoniae
What is the median age of onset of Whipple disease?
- 50 years
- 40 years
- 60 years
- 30 years
- 70 years
What are the endoscopic findings in Whipple disease?
- Clusters of distended villi
- Clustered giant cells
- Ulcerated, bleeding mass
- White linear scar
- Erythema and granularity
Author of lecture Whipple Disease

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
