Playlist
Show Playlist
Hide Playlist
Vesicoureteral Reflux (VUR) and Types of Reflux


-
Slides VUR Pediatrics.pdf
-
Download Lecture Overview
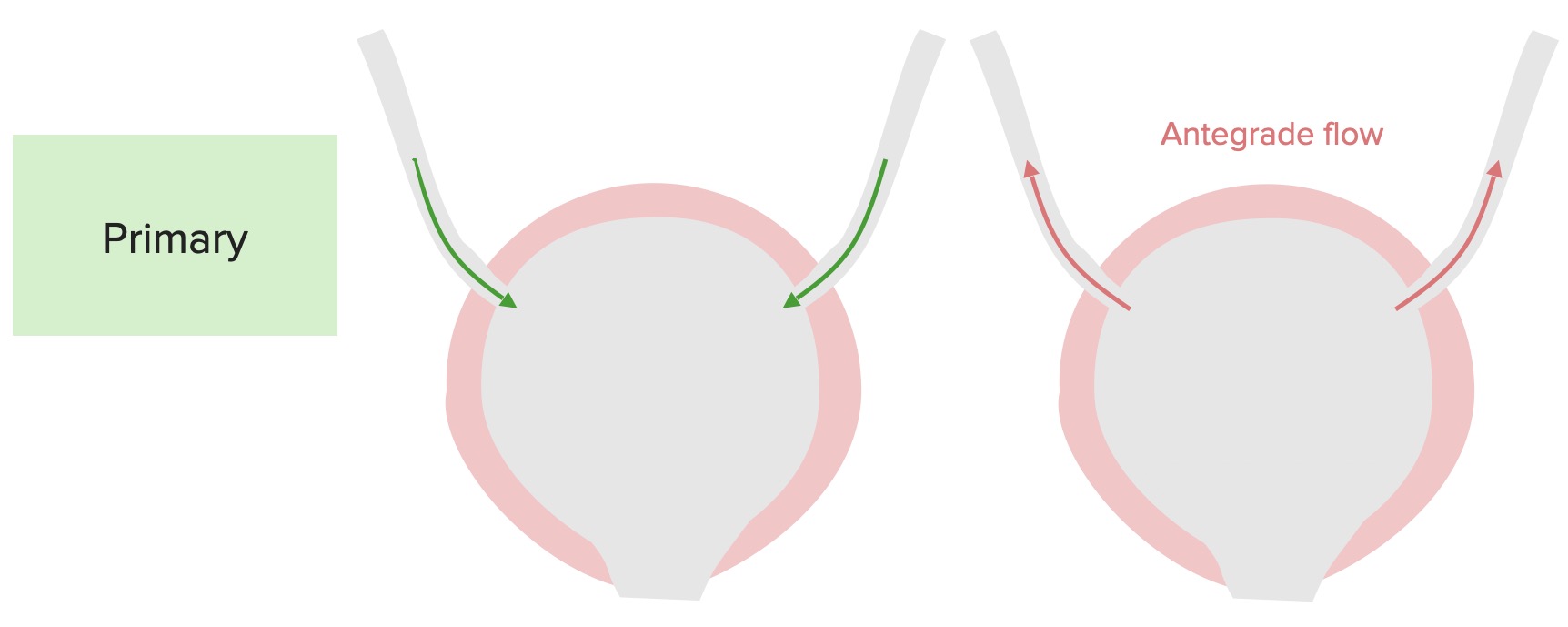
00:01 In this lecture, we’re going to discuss vesicoureteral reflux. 00:07 So this is a very controversial conversation to be having. 00:12 Several people feel passionately about vesicoureteral reflux one way or the other in terms of how important it is to both recognize it and to treat it. 00:22 But I’m going to weigh it in there anyway. 00:24 So vesicoureteral reflux is essentially a refluxing of urine out of the bladder and back up towards the kidney. 00:34 Essentially, for reasons that are diverse, as a child tries to pee, the urine may come out a little bit but much of it is going backwards up the wrong way and back into the kidney. 00:46 There are five different types of vesicoureteral reflux and we typically historically have graded them thus. 00:55 We have grade I vesicoureteral reflux, where it’s going just up into the ureter. 00:59 Grade II where it does the entirety of the ureter. 01:02 Grade III where we start seeing changes in the calices, in the urine collecting system of kidney. 01:08 Type IV where we really starting to see significant renal damage and grade V which is what we might call a mega ureter. 01:16 A huge ureter that goes up and back into the kidney. 01:20 What’s interesting about this is vesicoureteral reflux of all types may well completely resolve of its own in childhood. 01:31 In fact, the majority of grades I and II will completely resolve on their own, about half of grades III and then the minority of grades IV and V. 01:41 But it is remarkable that roughly 1 in 8 patients with grade V mega ureters will completely resolve on their own as they grow through childhood. 01:52 So vesicoureteral reflux when it’s severe, and the reason why we’re concerned about it, can cause renal scarring. 02:01 This scarring will cause areas of the kidney that don’t work correctly. 02:06 And as you know, eventually if we keep running out of kidney, we end up in renal failure or with hypertension. 02:15 So it’s important to know how much renal scarring is going on in these children as there is a theoretical concern they could end up much later in life with severe kidney disease. 02:27 So for the last 20 years, we have understood a few things to be true. 02:32 We have noted that children with reflux are more likely to get pyelonephritis. 02:38 These children with reflux are more inclined to get kidney infections because they’re inadequately emptying their bladder and because that potentially bacteriuric urine in the bladder is going backwards up to the kidneys. 02:53 We also historically have said that recurrent pyelonephritis or recurrent kidney infections could cause worse scarring of the kidneys. 03:03 And we have said that pyelonephritis induced scarred kidneys could result in adult renal dysfunction. 03:12 These are may be sometimes true statements. 03:15 However, what we’ve discovered in some studies is that when we look at adults with end-stage renal disease or bad glomerular filtration rates, virtually none of them have that as a result of recurrent childhood pyelonephritis. 03:32 So that third point probably isn’t true. 03:36 The other thing we know is that while it’s true that recurrent pyelonephritis causes scarring of the kidneys, it’s not clear that it’s the pyelonephritis that is at fault and not the vesicoureteral reflux that’s causing pyelonephritis. 03:52 Or perhaps, it’s some other underlying element of the kidney that’s going on that causes it to scar easily. 03:59 So these last two points are somewhat controversial and we really can’t say for sure what exactly is going on. 04:09 But when we look at vesicoureteral reflux, it’s nice to be able to decide whether this is a primary problem or a secondary problem. 04:17 In other words, do they just have reflux or is there another structural problem that we might be able to fix that’s causing the reflux itself. 04:26 Let me be clear, primary vesico reflux looks like this. 04:31 Here, we have a normal bladder with two normal ureters coming in to the bladder. 04:37 And you can see the urine is flowing through a slightly angled area down into the bladder. 04:44 The reason that tube slightly changes direction as it goes through that bladder wall is because when the child decides to pee and squeezes that bladder, the muscle action squeezing the bladder also kinks off those ureters. 05:00 This prevents a natural back flow of urine and directs the urine instead out of the body. 05:07 In a patient with primary vesicoureteral reflux, the problem is really that these tubes go straight in. 05:15 They fail to angle slightly as the ureters travel through the bladder wall. 05:20 As a result, when this child tries to bare down and have a micturition, the urine will also flow backwards up into the kidneys. 05:32 This is usually unilateral but it can be bilateral or it could be bilateral with different grades, grade I on one side and grade III on the other for example. 05:43 Secondary vesicoureteral reflux happens as a result of a problem somewhere else in the tract. 05:50 An example would be posterior urethral valves. 05:54 That happens to boys and we’ll talk about in a little more on. 05:58 Or ureteral-pelvic junction obstruction, that’s an obstruction higher up before the ureter even gets to the bladder. 06:06 Patients may have a neurogenic bladder. 06:08 We see this for example in spina bifida where their bladder isn’t capable of constricting right and as a result, urine can go backwards. 06:17 We also sometimes see it in renal transplants when they have to physically put the ureter into the bladder.
About the Lecture
The lecture Vesicoureteral Reflux (VUR) and Types of Reflux by Brian Alverson, MD is from the course Pediatric Nephrology and Urology. It contains the following chapters:
- VUR
- Types of Reflux – VUR
Included Quiz Questions
Which of the following statements is TRUE about vesicoureteral reflux?
- The majority of type I and II will resolve on their own without therapy.
- It is not associated with urinary tract infections.
- It is associated with deletion of the 22q11 chromosome.
- Type V is the most benign type.
- It typically occurs during periods between urination.
Which of the following types of vesicoureteral reflux is called mega-ureter?
- Type V
- Type I
- Type II
- Type III
- Type IV
Which of the following is the major complication of vesicoureteral reflux?
- Pyelonephritis
- Renal stones
- Renal scaring
- Renal vein thrombosis
- Hypertension
Which of the following is NOT a secondary cause of vesicoureteral reflux?
- Acute cystitis
- Posterior urethral valves
- After renal transplant
- Neurogenic bladder
Author of lecture Vesicoureteral Reflux (VUR) and Types of Reflux

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
by Jalil Z. on 2021-03-08 for Vesicoureteral Reflux (VUR) and Types of Reflux Excellent lecture. An important topic in pediatrics. I'm glad it is explored in such details. Thank you!
Excellent lecture. An important topic in pediatrics. I'm glad it is explored in such details. Thank you!
