Playlist
Show Playlist
Hide Playlist
Leukemia: Types of Leukemia incl. Hairy Cell Leukemia (HCL) and Adult T-Cell Leukemia/Lymphoma (ATLL) – White Blood Cell Pathology

-
Slides Leukemia White Blood Cell Pathology.pdf
-
Download Lecture Overview
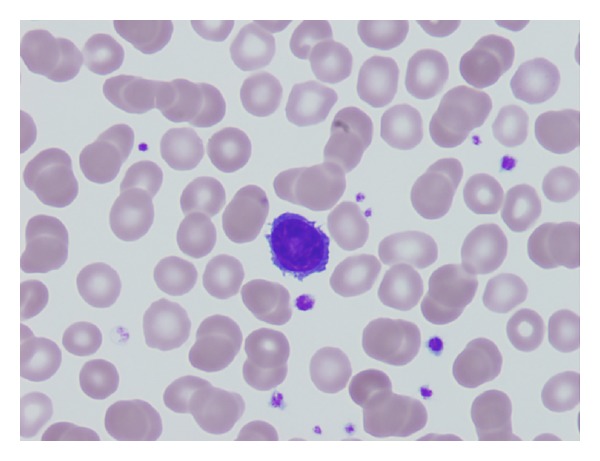
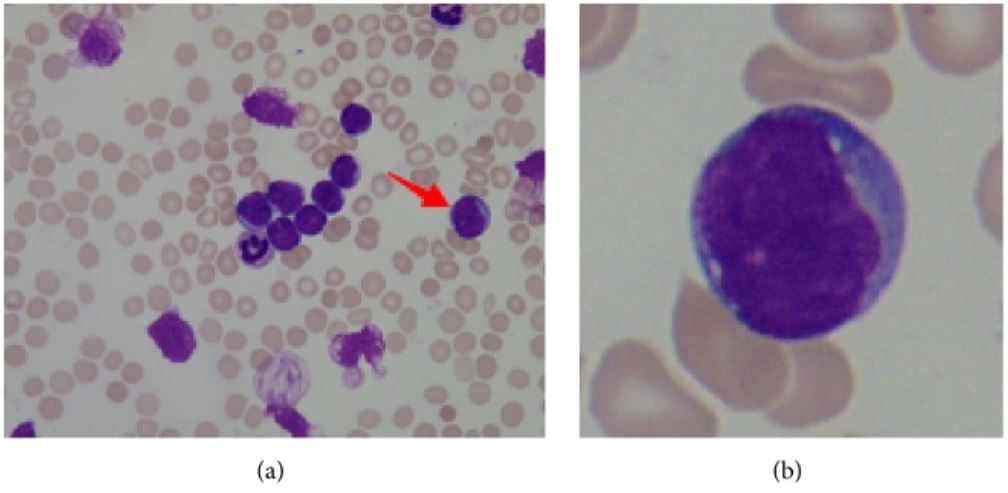
00:02 Ultimately, this table gives you the highlights of what you need to know for your leukemias. 00:07 We’ve walked through every single one in great detail, and now at this point, let’s quickly walk through what you need to know from comparing one from the other. 00:15 Age: Children affected by leukemia, ALL. 00:20 The oldest patient to be affected with leukemia, CLL. 00:25 Forties, CML. 00:28 AML, all over the place, 15 to 60. 00:32 Onset, acute/acute. 00:35 What does that mean? In your bone marrow, you'll find greater than 20% blasts. 00:39 What was that pre-leukemia that I told you about AML? That was myelodysplastic syndrome. 00:44 Do not forget that. 00:46 And in RBC pathology, I’d also discussed it. 00:49 There’s a variant that you want to know known as refractory anemia, a ring sideroblast. 00:54 Chronicity, well, chronic. 00:56 You would have less than 10% blast in the bone marrow. 01:00 CLL associated with SLL, aggressive form, Richter transformation. 01:06 CML, aggressive fashion. 01:08 What is that called? Blast crisis. 01:11 Symptoms, acute: bone, bone, bone pain. 01:15 That’s what you pay attention to because of infiltration of bone marrow. 01:18 If it’s chronic, many times, nonspecific but anemia type of symptoms. 01:24 Prognosis: ALL, excellent. 01:28 What kind? Pre-B type. 01:31 Pre-T, a killer. 01:33 AML, moderate. 01:35 If you’re dealing with M3, 30% cured, by? ATRA. 01:40 CML, pretty decent, especially when you can use imatinib. 01:44 The trade name is Gleevec, the generic name is imatinib. 01:49 And CLL, poor and slowly progressing, unless it goes into Richter transformation, which is now known as your diffuse large B-cell lymphoma. 02:01 Here, we have hairy cell leukemia. 02:02 Allow the name to speak to you. 02:04 This is once again of B-cell origin but it is rare. 02:07 Older males, splenomegaly. 02:09 I’m going to give you the highlights of what you want to take a look at. 02:12 You want to specifically look for monocytopenia. 02:15 That is an interesting and unique description that you do not find with most leukemias. 02:20 Monocytopenia. 02:22 Complications include opportunistic infections and vasculitis. 02:26 It is quite responsive to purine nucleoside analog. 02:30 And also keep in mind that the molecular trigger or what’s known as the molecular marker for this will be called B-Raf, and do not forget that. 02:40 Of course, TRAP as well, tartrate-resistant acid phosphatase. 02:44 But then B-Raf, you’re going to find almost 100% of your patients. 02:48 If you take a look at the cell here, there was no other cell. 02:52 With leukemia, a B-cell that looks like this in which it looks like hair-like projections. 02:57 Hence, it’s called hairy cell leukemia. 02:59 This is a B-cell, please do not forget that. 03:04 Our topic here is adult T-cell leukemia/lymphoma. 03:08 Remember, please, that you could have development of the cancer within your bone marrow. 03:13 Spills over into circulation, and then you go on to then affect your lymph node. 03:17 Here, we have adult T-cell leukemia/lymphoma. 03:20 You pay attention to T. 03:22 When you have a T-cell type of cancer, this would mean that you have skin involvement. 03:26 That’s exactly what happens here. 03:27 Not only would you have skin involvement but then you also have bone involvement, as we should describe in a second. 03:34 There’s a retrovirus that you need to make sure that you know of called your human T-cell lymphotropic virus. 03:40 This is a virus that is then going to cause damage, and may then give rise to your patient. 03:46 The endemic areas of HTLV-1 include Japan, Caribbean, and Central Africa. 03:51 There are some other places but those are the three big regions. 03:55 The disease is long latency, and decades after infection may will then result in the leukemia/lymphoma There is going to be widespread involvement of lymph nodes, and adenopathy and peripheral blood, and the skin is oftentimes involved. 04:10 In addition, there’s also a bone involvement as well with adult T-cell leukemia/lymphoma. 04:14 Unfortunately, the prognosis is quite poor. 04:18 Opportunistic infections are usually what the patient is going to die from. 04:22 Adult T-cell leukemia/lymphoma, T-cell, HTLV-1, tax, molecularly, if you remember, and we’re looking at skin issues, endemic.
About the Lecture
The lecture Leukemia: Types of Leukemia incl. Hairy Cell Leukemia (HCL) and Adult T-Cell Leukemia/Lymphoma (ATLL) – White Blood Cell Pathology by Carlo Raj, MD is from the course Leukemia – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following types of leukemia is most commonly seen in children?
- Acute lymphoblastic leukemia
- Acute myeloid leukemia
- Hairy cell leukemia
- Chronic myeloid leukemia
- Chronic lymphocytic leukemia
Which of the following types of leukemia has an excellent prognosis?
- Acute lymphoblastic leukemia
- Chronic lymphocytic leukemia
- Acute myeloid leukemia
- Acute T-cell leukemia
- Hairy cell leukemia
Author of lecture Leukemia: Types of Leukemia incl. Hairy Cell Leukemia (HCL) and Adult T-Cell Leukemia/Lymphoma (ATLL) – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Overall great series of the major points and he made it Dr. Raj made it intuitive and memorable.
