Playlist
Show Playlist
Hide Playlist
Supra- and Infraspinatus Muscles

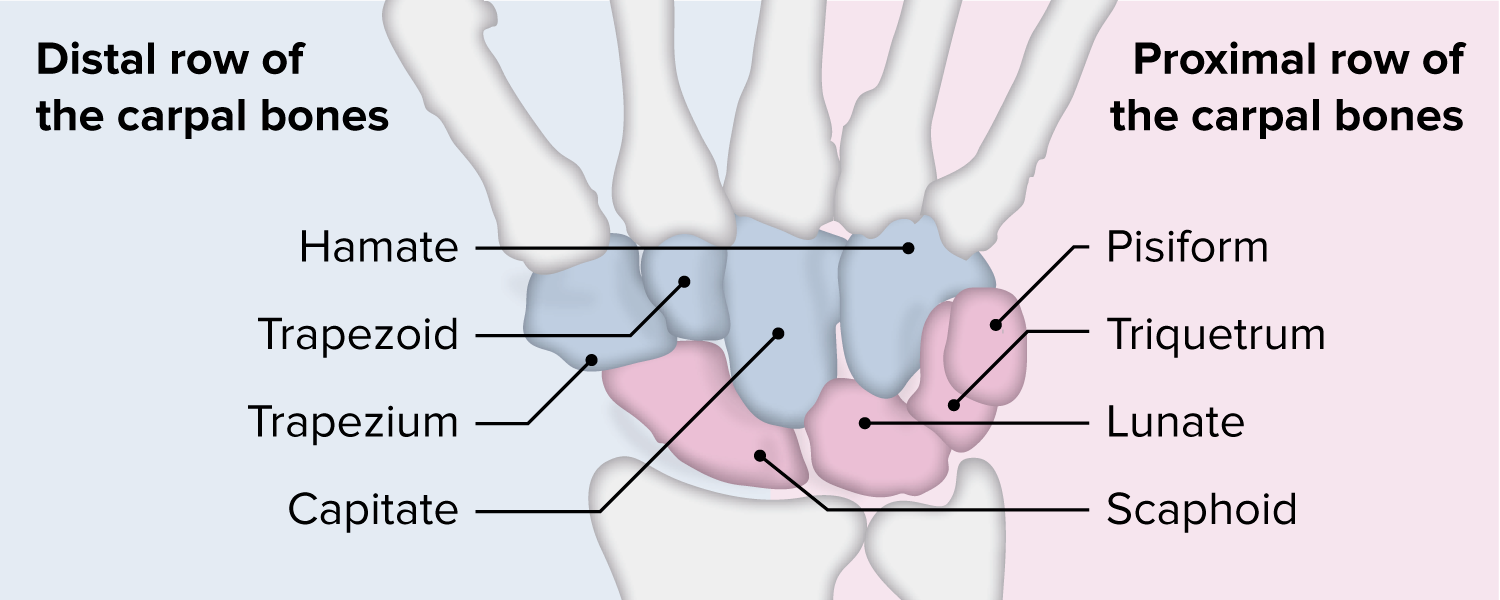
00:01 Okay. So, that’s the spine of the scapula, supraspinatus, infraspinatus, what supply those muscles? Well, the suprascapular nerve. 00:14 Very good. Where does it come from? From the first trunk. 00:18 Very good, from the upper trunk. From the upper trunk, you also have something called the suprascapular nerve. The suprascapular nerve supplies the supraspinatus and the infraspinatus.So that’s the supraspinatus, infraspinatus. Okay. That’s the edge of the scapula, what muscles are these? Teres minor and teres major. So teres minor is up there and teres major is up here. Nerve supply to teres minor? Axillary? Very good. Teres minor is by axillary, and teres major is by-- Lower subscapular. So the lower subscapular nerve supplies subscapularis, as well as teres major. Axillary nerve supplies deltoid, as well as teres minor. And then you have radial nerve. So the radial nerve supplies the triceps, I said. So the radial nerve -- you can see the spiral groove in him quite nicely. So there’s the spiral groove. It comes down. That’s the brachioradialis. 01:56 In the cubital fossa, if you reflect the brachioradialis, you will see the radial nerve there. Then it lies between the two heads of the supinator muscle. It runs between the two heads of the supinator there. And about seven centimeters, distal to the joined line, it divides into what? Posterior interosseous nerve. 02:23 Posterior interosseous nerve, and superficial brand of the radial nerve. Okay. So at this point, it divides into a posterior interosseous nerve, which is a deep branch similar to your anterior interosseous nerve which is also deep branch. And then you have the subcutaneous nerve which is called the superficial branch of the radial nerve. That’s what you’re testing for sensation. Now, posterior interosseous nerve. Nerve injuries. You will get a full EMQ on nerve injuries. So the favorite questions are related to levels of nerve injuries. Imagine your radial nerve is injured at this level, above the spiral groove, then the entire extensor aspect is paralyzed, quite obvious. If it is below the spiral groove, triceps is spared. So the patient will have extension of the elbow but wrist drop, below the spiral groove. Okay. Let’s go slightly lower down. At this level, what muscles are spared? Triceps is spared, fine, anything else? Which one? Brachioradialis. Brachioradialis is spared because the brachioradialis is supplied earlier than that. Then you have the anconeus which will be spared. Probably, we’ll also have the extensor carpi radialis longus and the brevis, which extends the wrist this way. That is also spared. When it comes down, the posterior -- before it gives off the posterior interosseous nerve at this level, always the extensor carpi radialis longus extensor carpi radialis brevis, anconeus, supinator, and brachioradialis. They’re always supplied. So if the patient has got a posterior interosseous nerve injury following a laceration, the patient would have a wrist-drop. The patient will be able to lift the wrist-drop, but there is loss of extension of the fingers. Okay. 04:24 So if you get a clinical scenario whereby they have all these different nerves and then the question says, “The patient is able to extend the wrist but not the fingers, which nerve is it?” It’s on the posterior interosseous nerve. Okay. It’s the posterior interosseous nerve. And the question will be a bit more specific. It will say, “The patient is able to extend the wrist but with radial deviation” because only the extensor carpi radialis longus and brevis is working. Now, the extensor carpi ulnaris. 04:55 So when the patient extends the wrist, the radial deviates. Because when you’re extending the wrist, you have the extensor carpi radialis on the radial side and extensor carpi ulnaris on the ulnar side working to extend it. So if posterior interosseous nerve is injured, the extensor carpi ulnaris is affected but not the radialis. So the patient can do this but it will deviate to the radial side. Staying on the radial nerve, it supplies all the other muscles in the hand, the thumb. What they’re going to ask you, you clearly know the names, extensor pollicis longus, extensor pollicis brevis, and then you have the abductor pollicis longus in the base of the snuffbox. Then to the digits, you should know the names, extensor digitorum communis, extensor indicis, and extensor digiti minimi. 05:55 There’s not really any EMQ question on that but you can get a question on the snuffbox, boundaries and contents of the snuffbox. Boundaries of the snuffbox? EPL. Yup, very good, on which side? On the ulnar side. Ulnar side? On the ulnar side, you have the extensor pollicis longus. And then there’s EPB on the medial side. 06:23 Extensor pollicis brevis and -- I can’t remember. 06:28 Abductor pollicis longus. So two longus and one brevis. On the ulnar side, this one -- So that is your extensor pollicis longus on the ulnar side. That’s the extensor pollicis brevis. 06:49 And then here is the abductor pollicis longus which abducts the thumb. Those are the boundaries of the snuffbox. Okay. What were the important structures here out of the snuffbox? So, the superficial brand of the radial nerve? Radial artery? Radial artery. Radial nerve is deep. Okay. Radial artery is deep and cephalic vein. They’re on the snuffbox. What are the bony prominences you can feel in the snuffbox? If you feel your snuffbox, clearly, you will feel the scaphoid. What else can you feel? Lunate? No. 07:28 Trapezium. Trapezium. Scaphoid, trapezium. Four bones, scaphoid, trapezium, anything else? Base of the first metacarpal and the radial styloid. 07:40 These are the four bones in the snuffbox. That’s the radial styloid -- Those clusters in the snuffbox, isn’t it? Yeah, that is it. Because if you look at the anatomical specimen, these tendons lie on these sites. Okay. So that’s the snuffbox. 08:00 So that’s all about the radial nerve. If you go back here, that’s your teres minor. 08:13 Where does the teres minor insert? Radial tuberosity. 08:22 Radial tuberosity of the humerus, okay. What else inserts along with the teres minor in the great -- Supraspinatus. 08:29 Very good. So supraspinatus, infraspinatus, teres minor. The rotator cuff muscles, so SITS, supraspinatus, infraspinatus, teres minor, they are attached the greater tubercle. 08:44 And the subscapularis is attached to the lesser tubercle. Those are the rotator cuff muscles. 08:52 So this is the teres minor. Where does the teres major insert? Think about it. 09:03 I’m sure you know this. If you can see the arm, the teres major coming from there, where can it insert? Think about it. It has to be in the shaft of the humerus. Where else can it go to? It has to, isn’t it? Because if it does not go into the shoulder, it has to be coming here. So it inserts into the medial lip of the bicipital groove of the humerus. 09:30 What else attaches there? That’s the biceps and that’s the bicipital groove. What are the muscles that are attached there? I’m sure you know this. Not biceps. 09:54 Triceps. No, no, no. Triceps all go to the olecranon, here You have the teres major, pectoralis major, and then your latissimus dorsi. 10:09 So that is a lady between the two majors; latissimus dorsi, pectoralis major, and teres major. 10:18 So your action of latissimus dorsi, pectoralis major, and teres major would have to be adduction of the arm. Okay. So these are your three muscles inserted here. So that’s the teres minor and teres major. I’ve drawn a quadrangle here. That is called the quadrangular space. Quadrangular space is essentially bounded laterally by the humerus, medially by the long head of triceps, teres major, teres minor. Okay. What comes out through this quadrangular space? Axillary nerve. 11:08 Axillary nerve, very good, axillary nerve, along with an artery. Go on. 11:18 Posterior -- Posterior circumflex humeral artery. So, the axillary nerve is accompanied by the posterior circumflex humeral artery. Whenever I try to emphasize something, that’s because this is what comes up; axillary nerve, posterior circumflex humeral artery. Then this comes down and then it becomes a triangular interval. 11:39 So the triangular interval is bounded superiorly by the teres major, along with the triceps, humerus. And what comes out through that? Radial nerve. So that is the radial nerve which is coming out through there and lying in the spiral groove. Which artery accompanies that? The profunda brachii. 12:05 Profunda brachii artery, very good. Where does the profunda brachii artery come from? The axillary, the brachial -- Brachial artery. I think at this point, I’ll tell you something which is of quite relevance. I said this is the teres major, right? The anatomical significance of that point is your axillary artery comes there. At this point, it changes name, and then it becomes the brachial artery. So that’s an anatomical point where the name changes. So the moment it becomes the brachial artery, it immediately gives off the profunda brachii branch. So if you go back to this image here, that’s where you get the profunda brachii immediately coming off below the teres major. So axillary artery runs down, comes below the teres major, and immediately given off the profunda brachii branch, and then the brachial artery just continues into the arm. Whenever you say profunda, profunda is deep. So it supplies the deep muscles in the arm. Okay, So don't refer to your quadrangular interval, boundaries, contents. Sorry, quadrangular space. Triangular interval, boundaries, contents. 13:39 So, going back here, radial nerve, we discuss axillary. Axillary nerve, just remember your deltoid. You have the anterior fibers, lateral fibers, and the posterior fibers. 13:58 They’re all supplied by the axillary nerve, and this is a little bit more detail. Axillary nerve has got an anterior and the posterior division. That’s why one-off it supplies the teres minor. But for part A, don’t confuse which is anterior and which is posterior. 14:16 Just remember that teres minor is also supplied by the axillary nerve. And the axillary nerve sensory is the regimental badge area, which I’m sure you know this. That’s your sensory distribution for axillary. It’s very difficult to test for teres minor in isolation because it’s a part of the rotator cuff. So, whenever you’re asked any shoulder pathology, this always comes along with supraspinatus, infraspinatus, and teres minor is part of it. It’s because you just can’t isolate spontaneously. Subscapularis, you can because it’s coming out attaching on the lesser tubercle. Okay. Now, we briefly
About the Lecture
The lecture Supra- and Infraspinatus Muscles by Stuart Enoch, PhD is from the course Musculoskeletal - Upper Limb.
Author of lecture Supra- and Infraspinatus Muscles

Stuart Enoch, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
