Playlist
Show Playlist
Hide Playlist
Subarachnoid Hemorrhage: Management


-
Slides Head Trauma Subarachnoid Hemorrhage.pdf
-
Download Lecture Overview
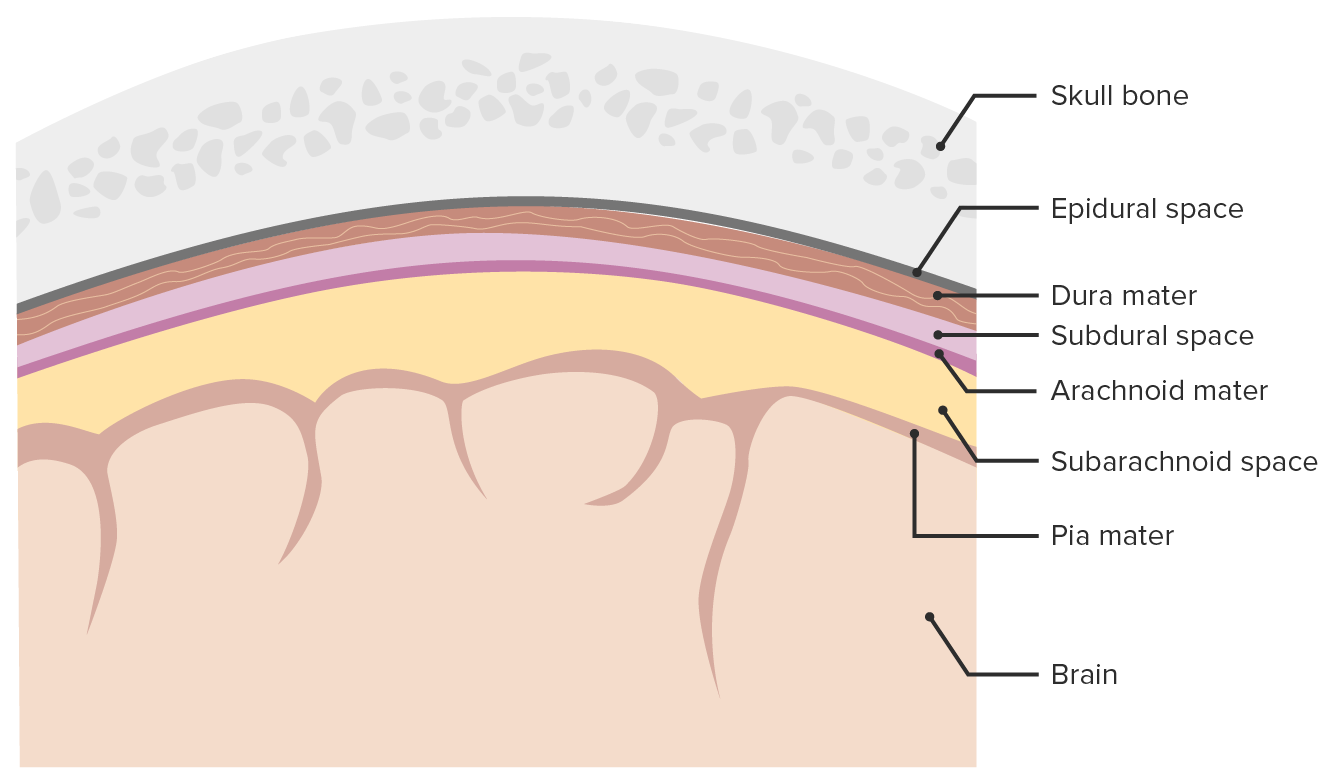
00:01 How do we manage these patients? For patients with both moderate and severe subarachnoid hemorrhage, this can result in life threatening conditions and those patients need to be stabilized in the hospital or in the ICU. 00:15 First we want to address any trauma that may have occurred, address blood, blood loss due to anemia or any internal organ damage that may have occurred from trauma. 00:23 We need to secure the airway and patient with reduced Glasgow Coma scales who are unable to protect their airway. 00:31 Normalization of cardiovascular abnormalities is important. 00:34 We can see troponin elevations in these patients as a result of the cerebral stress from the subarachnoid hemorrhage. 00:40 We want to manage arrhythmias and stabilize blood pressure. 00:43 Discontinuing antiplatelet or anticoagulant medications and anticoagulants need to be reversed in this patient population, and treat seizures if they occur. 00:53 In addition, a concerning complication that we can see in patients with subarachnoid hemorrhage is vasospasm. 00:59 The blood is in the subarachnoid space and this is also where blood vessels course through. 01:05 That blood is an irritant and can result in vasospasm or compression and narrowing of blood vessels and contribute to stroke. 01:13 Classically, we would consider two ways to prevent vasospasm and patients with subarachnoid hemorrhage and we may consider pressors to do that. 01:20 We want to increase total body fluid and we can use active resuscitation IV fluids to do that. 01:27 In addition, Nimodipine as a calcium channel blocker that we may utilize and frequently utilized to prevent and treat vasospasm in patients with subarachnoid hemorrhage. 01:36 Calcium channel blockers vasodilate, we want the blood vessels to be bigger, we want to prevent vasospasm and Nimodipine is a successful intervention. 01:46 To do that as often continued for 14 or even 21 days as the blood is resolving and we're moving outside of that window of vasospasm which can last up to 21 days following subarachnoid hemorrhage. 02:00 What about management surgically or endovascularly? Well, in many of these patients we consider consultation with neurosurgery, particularly in the setting of aneurysmal subarachnoid hemorrhage. 02:12 The goal of intervention is to stop the bleeding, prevent rebleeding manage increases in ICP and prevent secondary ischemia. 02:20 And we may consider a number of different surgical approaches. 02:24 We may clip an aneurysm or endovascularly coil an aneurysm, place a ventriculoperitoneal or ventriculostomy shunt to divert CSF in the cases of increased ICP. 02:36 And some patients may require a decompressive hemicraniectomy to manage underlying cerebral edema that can occur as a result of traumatic subarachnoid.
About the Lecture
The lecture Subarachnoid Hemorrhage: Management by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What fairly specific finding might a lumbar puncture show in a patient with subarachnoid hemorrhage?
- Xanthochromia
- Lymphocytic pleocytosis
- Albuminocytologic dissociation
- Oligoclonal bands
- Low glucose
What complication of subarachnoid hemorrhage is due to blood acting as an irritant?
- Cerebral vasospasm
- Seizure
- Brain stem herniation
- Coma
- Hydrocephalus
What pharmacologic treatment is effective in preventing vasospasm in patients with subarachnoid hemorrhage?
- Nimodipine
- Amlodipine
- Propranolol
- Diltiazem
- Mannitol
Author of lecture Subarachnoid Hemorrhage: Management

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
