Playlist
Show Playlist
Hide Playlist
Subarachnoid Hemorrhage (SAH – Emergency Medicine)


-
Emergency Medicine Bord Intracranial Hemorrhage.pdf
-
Download Lecture Overview
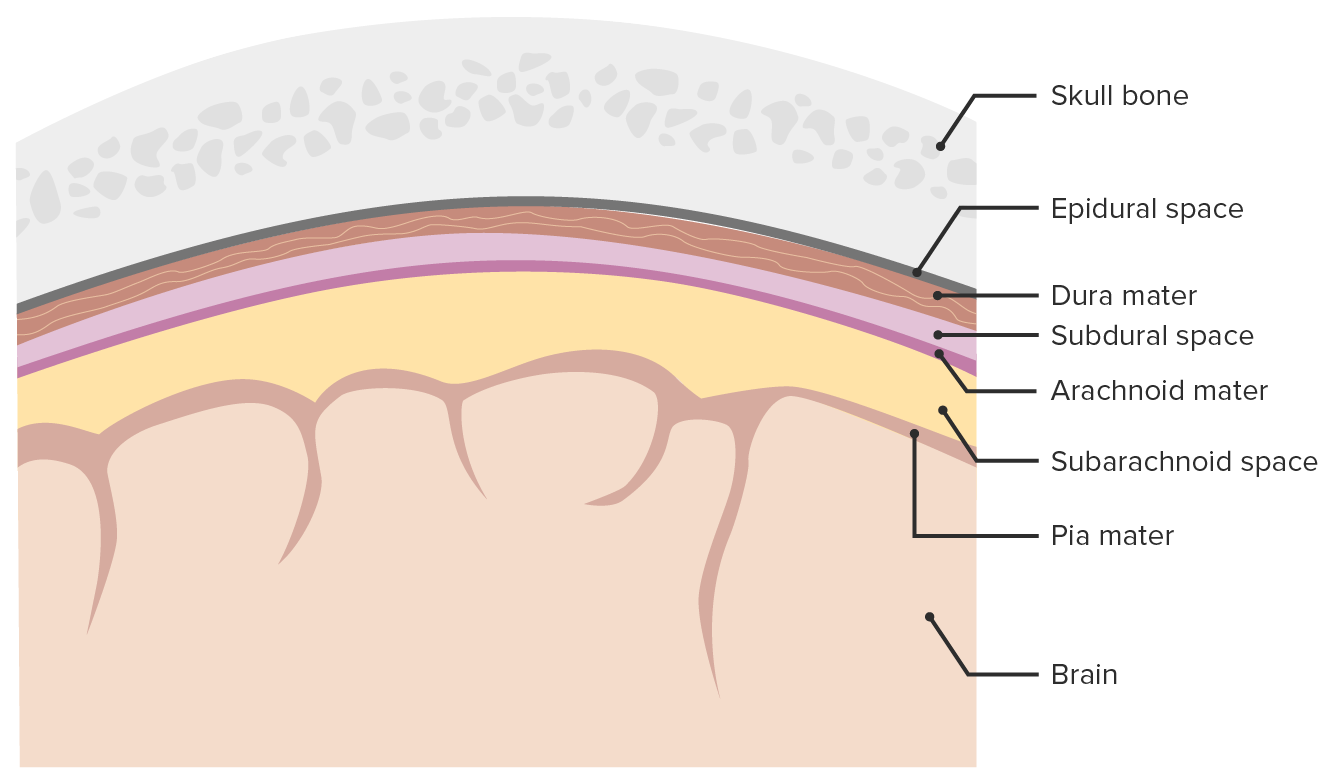
00:01 We’re gonna take a moment to move on and talk about the subarachnoid hemorrhage. 00:05 So subarachnoid hemorrhage is blood in the subarachnoid space and it accounts for 10% of all strokes. 00:12 It’s the most common cause of death related to stroke and the classic presenting thing here is that someone will develop a very severe sudden onset headache and by the time they even seek medical care, they already have severe and significant brain damage. 00:28 A saccular aneurysm is a cause 80% of the time and what that is basically is it’s a small aneurysm on one of the blood vessels. 00:36 Other causes can include AVM, mycotic aneurysms which are aneurysms caused by a fungus or a bacteria and finally neoplasms. 00:45 Most patients are between the ages of 40 to 60 years of age, so we’re not talking about very elderly people. 00:50 We’re talking about people who are generally middle aged. 00:53 There are some risk factors associated with subarachnoid hemorrhage developing. 00:58 One is hypertension, then smoking, excessive alcohol consumption and then sympathomimetic drugs, mainly cocaine being one of the key risk factors here. 01:10 There are also risk factors that are familial related. 01:14 This may seem a little bit kind of out of the blue, but actually it’s important to ask if there’s any history of polycystic kidney disease in the family. 01:23 Because the adult version of polycystic kidney disease is associated with subarachnoid hemorrhage development. 01:29 Other associated things are coarctation of the aorta, Ehlers-Danlos syndrome, as well as Marfan’s syndrome. 01:36 The latter two of these, it’s because it disrupts the wall of the blood vessels and can predispose to subarachnoid hemorrhage. 01:44 Patients who are presenting with subarachnoid, the classic history is that they have a thunderclap headache. 01:50 A thunderclap headache is a headache that peaks in seconds to minutes. 01:53 So you go from not having a headache at all to all of a sudden, having a sudden onset severe, severe headache. 02:00 The other classic thing that subarachnoid hemorrhage can be associated with is that it can be an exertional headache. 02:07 So if someone comes in and they told you that they got a headache when they were working out, when they were having a Valsalva maneuver which is if they were bearing down in some way, sexual intercourse, so classic is with climax, that they can potentially get a severe onset of headache in that situation. 02:22 Those are very classic things that are related to subarachnoid hemorrhage, so it’s important to try and get that information from patients if they’re able to communicate with you. 02:32 Other symptoms that may be related; nausea and vomiting, patients may pass out, there may be associated neck stiffness and that’s due to the fact if the meningeal system is irritated. 02:45 They may have photophobia, the light may bother their eyes. 02:49 And they also may present with seizures. 02:51 So you wanna make sure you’re trying to get as much of this information from patients to try and figure out how risky or how high risk their story is or their presenting history is for this chief complaint. 03:02 On the physical exam, you wanna assess for meningismus. 03:05 You can have the patient flex their neck and see if that causes pain. 03:09 You wanna assess their level of consciousness. 03:13 Sometimes these patients can present and already be very, very altered. 03:17 They might have a low GCS score. 03:19 And then you wanna think about their neurologic exam findings. 03:23 One of the classic things with subarachnoid hemorrhage is they can have disruption or alteration of their ocular motor nerves, so checking and making sure that their extra ocular movements are full and complete, and that they can move their eyes all around is a very key thing. 03:36 Now, I don’t wanna discount the fact also, you wanna pay attention to the airway, the breathing, and the circulation and you wanna make sure you’re paying attention to that ABC’s because those are always critical here and if your patient needs airway management, or is having a disruption in their breathing, you wanna make sure that you intervene on those in the appropriate time.
About the Lecture
The lecture Subarachnoid Hemorrhage (SAH – Emergency Medicine) by Sharon Bord, MD is from the course Neurologic and Psychiatric Emergencies.
Included Quiz Questions
Which of the following is the most common cause of non-traumatic subarachnoid hemorrhage?
- Berry aneurysm
- Arteriovenous malformation
- Mycotic aneurysm
- Neoplasm
- Angiomatosis
Which of the below is NOT a risk factor for subarachnoid hemorrhage?
- Hypotension
- Smoking
- Alcohol
- Sympathomimetic drugs
- Hypertension
Which of the following is a common symptom of subarachnoid hemorrhage?
- Photophobia
- Dyspnea
- Dysentery
- Hypotension
- Urinary incontinence
Author of lecture Subarachnoid Hemorrhage (SAH – Emergency Medicine)

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
