Playlist
Show Playlist
Hide Playlist
Stroke: Localization

-
Slides Stroke and intracranial hemorrhage.pdf
-
Download Lecture Overview
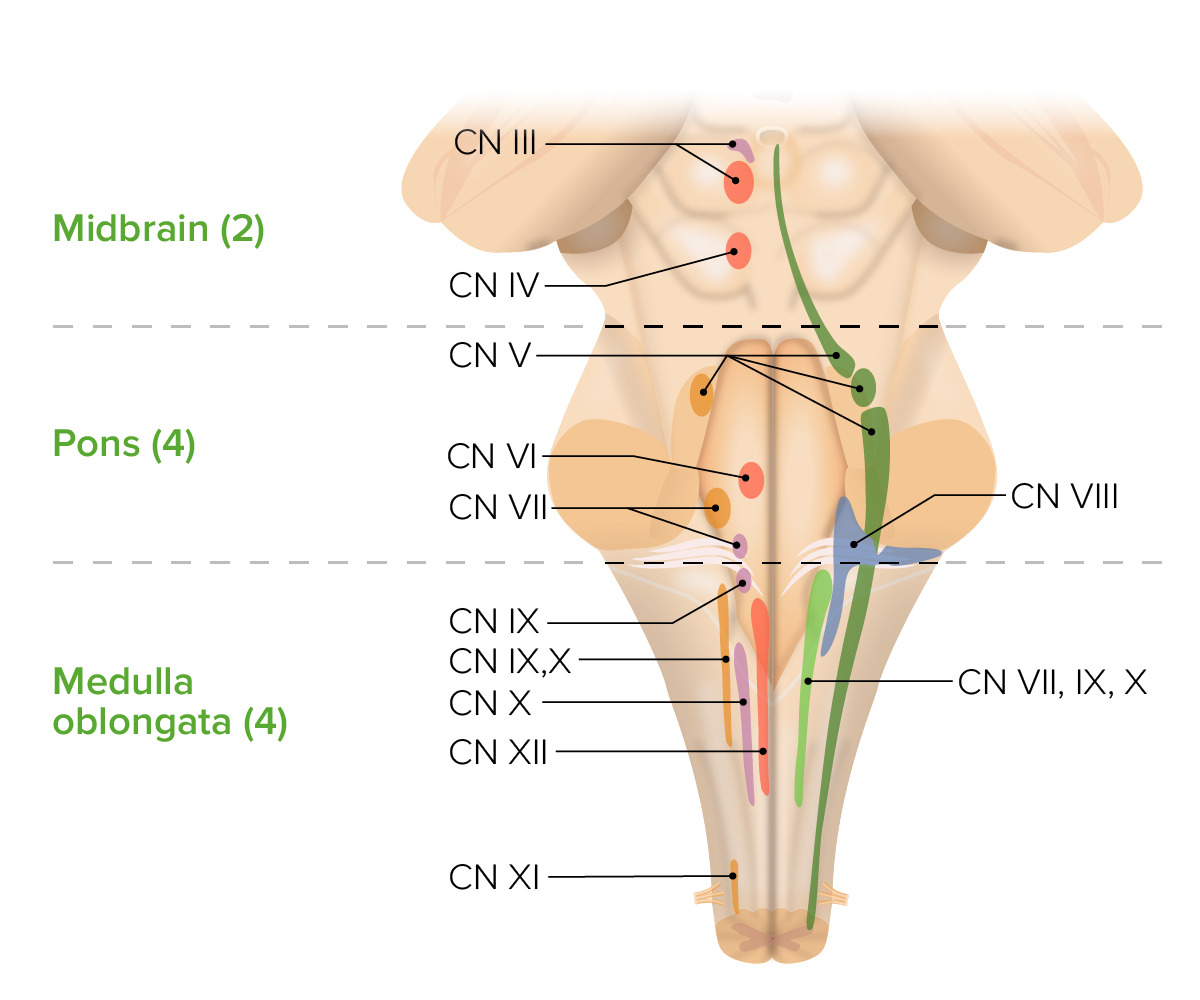
00:01 Let's take a couple of minutes to dive deep into the brainstem. 00:05 The brainstem is composed of 3 sections: the midbrain, the pons, and the medulla. 00:10 Let's look at the major nervous structures that exist in each of those 3 areas and think about the common strokes syndromes that would present with pathology in each of those areas. 00:23 We'll start with the midbrain. 00:25 The critical structures that you should know when considering a stroke in the midbrain are that this is home to cranial nerve 3, 4 and the vertical eyes center as well as strength on one side of the body or the other. 00:39 Here we can see cranial nerve 3 as it exits in the midbrain. 00:43 We see the nucleus of cranial nerve 3 line just medially. 00:48 At the posterior aspect or the dorsal aspect of that nucleus is the nucleus of the Edinger-Westphal, Edinger-Westphal nucleus which controls the parasympathetic fibers for cranial nerve 3. 00:59 And then importantly, the cerebral peduncles run on the ventral aspect of the midbrain. 01:05 And these are the critical structures to remember when we're considering a midbrain pathology. 01:11 Sometimes the medial lemniscus which controls sensory information is important and the spinothalamic track. 01:18 The spinothalamic tract controls pain and temperature, medial lemniscus is vibration and proprioception. 01:24 And those can help us to further localize a stroke in the midbrain. 01:29 So what types of stroke syndromes do we see? Well, we we need to remember cranial nerve 4 lies medially, the cerebral peduncles lie ventrally and the anterior lateral system lies laterally. 01:41 So there's 3 stroke syndromes to consider in the midbrain. 01:45 The first is a medial stroke syndrome. 01:48 And this is a stroke that affects those perforators, those pontine or midbrain perforators right off the basilar artery. 01:56 Medial strokes will affect cranial nerve 3 and the cerebral peduncles. 02:01 Patients who will be weak on one side of the body and on the opposite side, the side of the lesion will see a cranial nerve 3 palsy. 02:10 The second presentation is that of a lateral midbrain stroke. 02:13 There we often don't see cranial nerve 3 palsies but we do see problems with the anterior lateral system and the medial lemniscus in addition to varying degrees of weakness, involvement of the cerebral peduncles, the anterior lateral system and the medial lemniscus. 02:29 So we see hemisensory loss, motor weakness and we can see loss of both, pain, temperature, vibration and proprioception fibers. 02:38 If the entire side, if one entire side of the midbrain is involved, we see cross findings. 02:44 On the side of the lesion, the eye is down and out, there's a cranial nerve 3 palsy and that secondary to unopposed action of the 4th and 6th nerves when cranial nerve 3 isn't working. 02:56 Cranial nerve 3 also controls the parasympathetics and so that affected eye will be dilated and unresponsive. 03:03 That's a 3rd nerve palsy. 03:05 On the opposite side of the 3rd nerve palsy, the patient will have paralysis of the face, arm and leg as a result of dysfunction of the corticobulbar and corticospinal fibers that descend in the crus cerebri. 03:19 This is a critical stroke syndrome to be able to recognize, it's a midbrain stroke syndrome. 03:26 Let's go one section down to the level of the pons. 03:29 What things live in the pons that we need to be worried about for stroke patients that may have a pontine stroke? Well, the pons is home to cranial nerves 5, 6, 7 and 8 as you can see here. 03:41 It is the horizontal gaze center, that's where the PPRF or the pontine paramedian reticular formation lives and controls horizontal gaze. 03:53 In addition, we also see the corticospinal tract running in the ventral aspect of the pons which is critical, medial aspect strokes can cause weakness in this area, the medial lemniscus runs just dorsally to that and we can see those are the critical structures to evaluate when considering a pontine stroke. 04:13 So what are the major stroke syndromes we should recognize in the pons? Well, first is the medial syndrome. 04:21 Medial syndromes where the stroke involves the pontine perforators will affect the corticospinal tract primarily and result in contralateral weakness or hemiparesis. 04:33 Laterally we can see involvement of the 5th cranial nerve in contrast to the midbrain where cranial nerve 3 exits medially. 04:41 Cranial nerve 5 exits laterally as you see here, so we can see varying degrees of weakness and sensory loss in addition to sensory loss on one side of the face in the V1, 2 and likely 3 distribution. 04:54 In addition, there's one important structure that lives in the pons that can present with a unique stroke syndrome. 05:00 And that stroke's affecting the medial longitudinal fasciculus. 05:05 As you recall, the MLF connects the 6th nerve to the opposite 3rd nerve. 05:10 It allows our eyes to move together when we look laterally. 05:14 Strokes affecting or any pathology affecting the medial longitudinal fasciculus will cause the eye not to look in impaired adduction of the eye. 05:26 So when the patient tries to gaze right, a problem with the MLF will result in inability of the left eye to look right. 05:34 Or if the patient were to look to their left, a problem with the right MLF would cause an inability of the right eye to look left. 05:43 That's called an INO or an Internuclear Ophthalmoplegia and it comes from a problem with a medial longitudinal fasciculus or lesion in this case stroke in the pons. 05:55 And so when we think about pontine strokes or large pontine strokes, the two findings we want to think about, the crossed findings are on the side of the lesion, we see ataxia of the limbs, and gait abnormality as a result of loss of cerebellar fibers and the in pontine nuclei and that's on the side of the lesion. 06:13 Opposite the side of the lesion, we can see paralysis of the face, arm and leg as a result of impairment of the corticobulbar and corticospinal tract. 06:22 And variable impairment of touch proprioception as a result of medial meniscus involvement. 06:28 That crossed finding is important for localizing to a pontine stroke. 06:34 And finally, we get to the level of the medulla, the lowest part of the brainstem. 06:39 This is home to cranial nerves 9, 10, 11 and 12. 06:42 There's no eye movement involvement in the level of the medulla except problems in the medalla can cause nystagmus as a result of descending cerebellar fibers. 06:52 We can see prominent vertigo and nausea as a result of this vestibular nuclei involvement in the medulla. 06:59 We see crossed face body sensory loss And we can even see hiccups and yawning as a result of cranial nerve 10 and other autonomic cranial nerve function in the medalla. 07:11 Here are the critical structures include the spinal tracts of cranial nerve 10 and its nucleus. 07:19 The nucleus of cranial nerve 11 lies in the medulla. 07:22 The pyramids which carry the motor function in the cortical spinal tract are here and decussate here, so we can start to see crossed findings from a motor standpoint. 07:33 The lateral corticospinal tract is present in the medulla. 07:37 And we see the fasciculus gracilis and cuneatus which carry sensory nerve function, the dorsal column function, the vibration and proprioception in the dorsal aspect of the medalla. 07:51 So when we think about the important stroke syndromes in the medulla, we can have high medullary strokes in the cranial aspect of the medalla and low medullary strokes in the caudal aspect of the medalla. 08:04 In the upper part of the medulla, the corticospinal tract has not crossed over in the pyramidal decussation. 08:12 So we see that sensory loss and motor loss are on the same side, and that's contralateral to the lesion. 08:18 That's an important localizing finding. 08:21 We don't see corticobulbar dysfunction, and so facial loss, loss of motor function in the face or sensory function in the face are not present for a medullary stroke. 08:32 In a lower medullary strokes, after we've seen crossing of the corticospinal fibers at the pyramidal decussation, we see that sensory loss occurs on the opposite side as the motor loss. 08:45 Typically, we would expect the motor loss to be on the side of the lesion and the sensory loss to be opposite the side of the lesion. 08:53 In addition, we can see a varying range of parasympathetic dysfunction causing dizziness, nausea, vomiting, hiccups, and other parasympathetic and sympathetic dysfunction as a result of loss of cranial nerve 9, 10, 11 and 12 nuclear function. 09:10 And then lastly, we can divide the brainstem into the ventral portion of the brainstem and the dorsal portion of the brainstem. 09:18 The dorsal portion of the brainstem is home to the cranial nerve nuclei, that's where they live. 09:22 And so brainstem lesions can present without motor weakness and just cranial nerve nuclear weakness or lesions from problems affecting the dorsal aspect of the brainstem. 09:34 Typically, these are the deep perforating arteries of the basilar that are affected. 09:41 In the ventral aspect of the brainstem, that's home to the motor tracks, the corticospinal tract, the medial lemniscus tract. 09:48 So brainstem lesions involving only the ventral tracts can cause a pure motor hemiparesis usually with equal face, arm and leg if the pons is involved. 09:59 And there may be no other signs, no cranial nerve signs as a result of absence of dysfunction in the dorsal part of the brainstem. 10:09 And so here's a table that's an important reference as you're considering some of the major stroke syndromes, their vascular territory, and they're presenting signs or symptoms. 10:19 We see that left MCA strokes have a characteristic presentation, often with aphasia and hemiparesis and the other findings you see here. 10:28 In contrast, right MCA strokes don't involve aphasia, but present with similar hemiparesis and hemisensory loss and neglect and other right-sided brain symptoms. 10:40 Left PCA strokes frequently present with occipital dysfunction and visual impairment, visual field defects. 10:48 Similar to right PCA strokes, which present very similarly with visual field defects. 10:54 Vertebral strokes have a distribution that is deep within the brainstem and that medullary region. 11:00 And so we see the dizziness, vertigo, nausea, quadriparesis that are present in medullary strokes. 11:07 There are number of penetrating artery distribution strokes, the lacunar strokes, internal capsule, ventral pons and thalamus. 11:14 And you can see here some of the characteristic, signs and symptoms for each of those lacunar syndromes.
About the Lecture
The lecture Stroke: Localization by Roy Strowd, MD is from the course Stroke and Intracranial Hemorrhage.
Included Quiz Questions
What set of nerve fibers are responsible for movement in the limbs and trunk?
- Corticospinal tract
- Corticobulbar tract
- Spinocerebellar tract
- Medial lemniscus
- Fifth cranial nerve (CN V)
What set of nerve fibers are responsible for sensation to the ipsilateral side of the face?
- Fifth cranial nerve (CN V)
- Corticospinal tract
- Corticobulbar tract
- Spinocerebellar tract
- Medial lemniscus
What set of nerve fibers are responsible for movements of the face, head, and neck?
- Corticobulbar tract
- Fifth cranial nerve (CN V)
- Corticospinal tract
- Spinocerebellar tract
- Medial lemniscus
What set of nerve fibers are responsible for loss of touch and proprioception on the OPPOSITE side of the lesion (contralateral) in a pontine stroke?
- Medial lemniscus
- Spinocerebellar tract
- Corticospinal tract
- Corticobulbar tract
- Fifth cranial nerve (CN V)
What set of nerve fibers are responsible for touch and proprioception on the SAME side of the lesion (ipsilateral) in a pontine stroke?
- Spinocerebellar tract
- Medial lemniscus
- Corticospinal tract
- Corticobulbar tract
- Fifth cranial nerve (CN V)
What area of the brain is affected in a patient with a stroke and symptoms of aphasia, right hemiparesis, right homonymous hemianopia, and left head/gaze preference?
- Left middle cerebral artery
- Right middle cerebral artery
- Right pons
- Left pons
- Right midbrain
Author of lecture Stroke: Localization

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
