Playlist
Show Playlist
Hide Playlist
Labor Stage 2: Shoulder Dystocia

-
Slides Shoulderdystocia Obstetrics.pdf
-
Download Lecture Overview
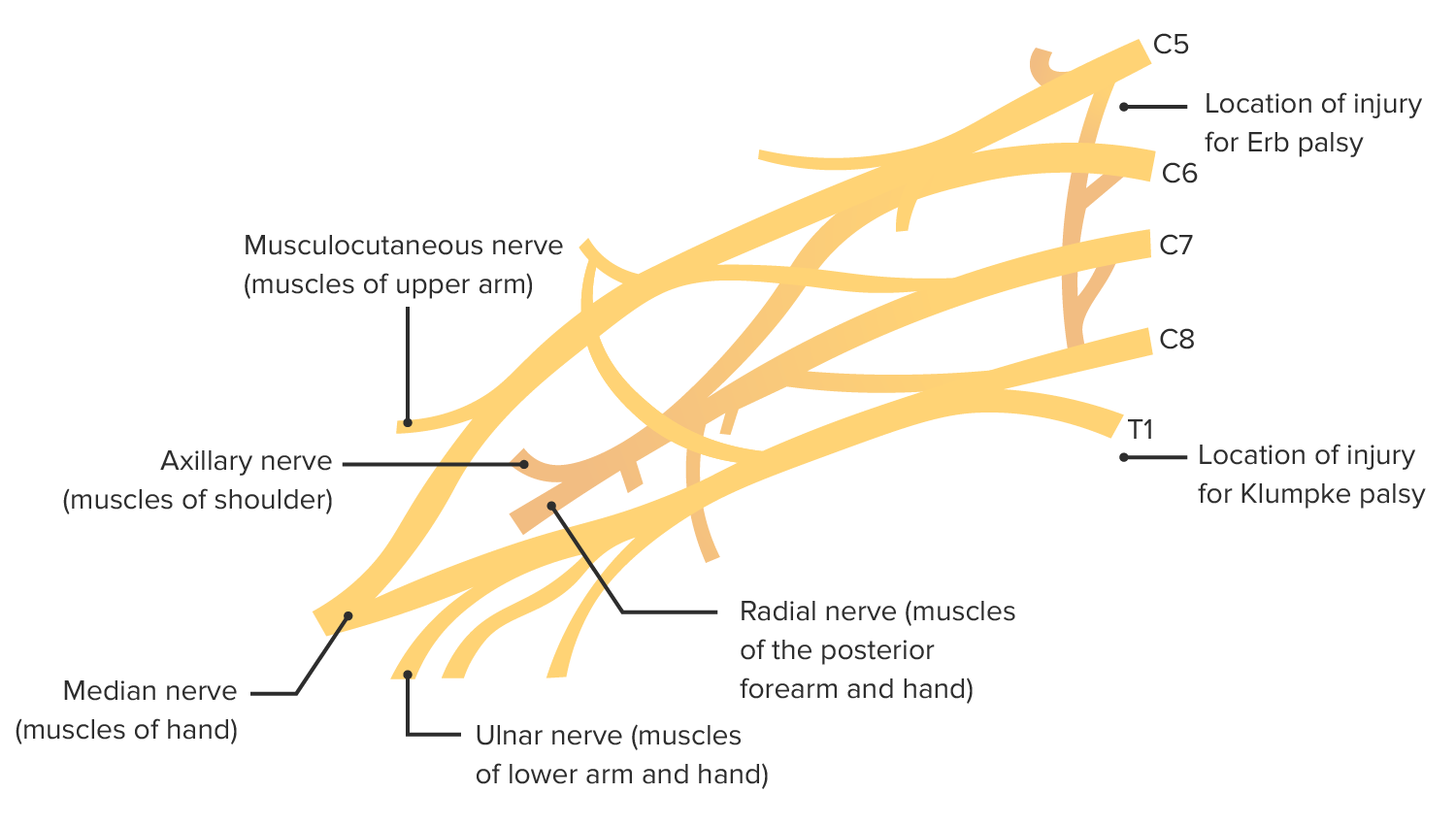
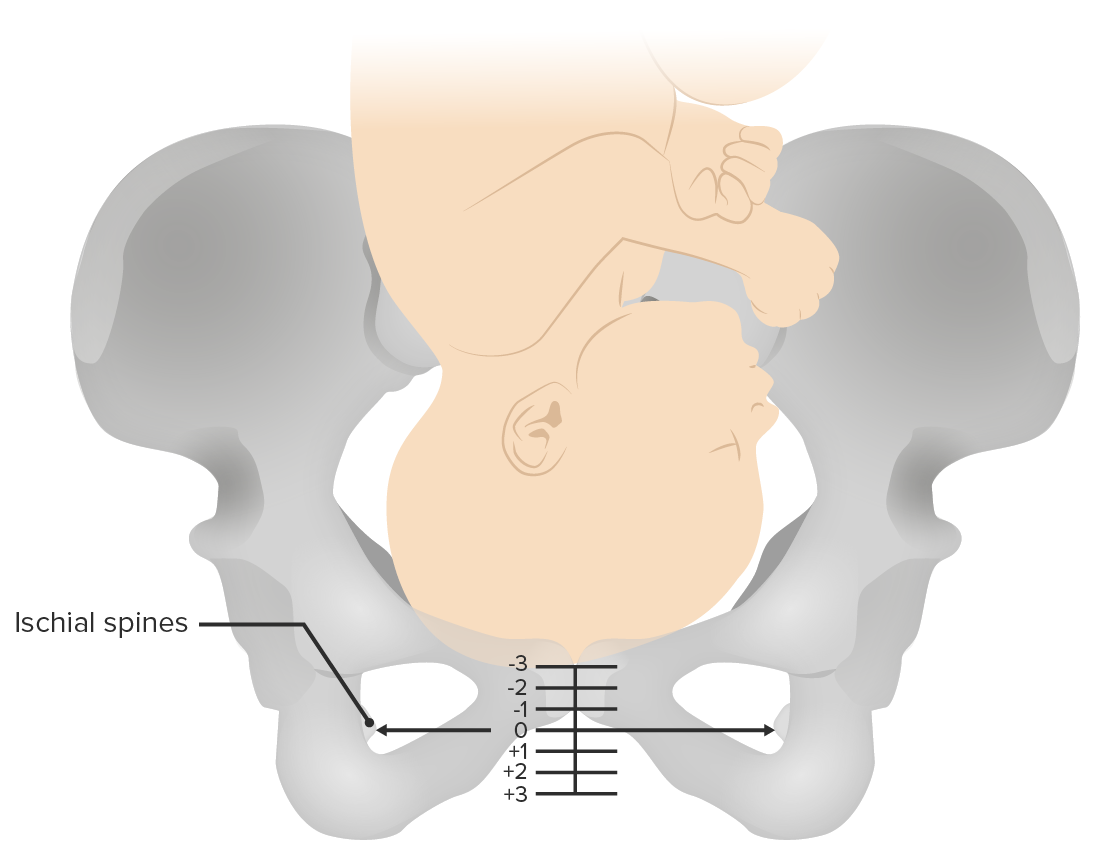
00:02 Now as part of abnormal labor, let's discuss Shoulder Dystocia. 00:07 So here's a clinical pearl. 00:09 Shoulder dystocias are unpredictable so you should always be prepared. 00:14 There are some signs that you can look for such as prolonged second stage of labor. 00:18 But any delivery has the potential to become a shoulder dystocia. 00:22 Any delivery requiring more than one routine maneuver to accomplish the delivery is considered a dystocia. 00:29 In a shoulder dystocia the anterior shoulder of the infant gets impacted behind the maternal pubic symphysis. 00:38 While shoulder dystocias can happen in any delivery there are some risk factors. 00:42 First, fetal macrosomia. 00:44 Next, maternal obesity. 00:47 Next a long second stage of labor in moms that are diabetic or have gestational diabetes. 00:53 There's an increased risk of shoulder dystocia. 00:55 And if a mom have a history of shoulder dystocia in a previous pregnancy, she's increased risk during that pregnancy. 01:04 So this is an ominous sign. 01:06 It's called the Turtle Sign. 01:08 And you can see here the chin is retracted against the maternal perineum and that's because the anterior shoulder is stuck behind the pubic symphysis. 01:16 This causes the head to recoil after delivery. 01:21 So what do we do when we see a shoulder dystocia. 01:23 Where's here is a mnemonic to help you. 01:25 It's called HELPERR. 01:26 First you want to call for help. 01:30 So when you are doing that delivery and you see that the anterior shoulder is not delivering, or you see the turtle sign that we discussed, you have a shoulder dystocia and you should call for Help. 01:39 Help means calling other nurses in the room. 01:42 Calling for an additional obstetrician and possibly contacting your anesthesiologist. 01:47 The next thing to do is consider an Episiotomy. 01:52 Now I say consider an episiotomy because we have to remember that a shoulder dystocia is not a skin dystocia. 01:58 However, depending on the size of the infant and depending on the hands of the physician, you may need to consider cutting an episiotomy to be able to fit the hands in and do those additional maneuvers that we are going to discuss. 02:12 Next is lower the head of the bed and elevate the legs. 02:15 So what that means you lower the head of the bed so that mom's back is flat. 02:21 Elevate the legs means that you flex the knees towards the chest. 02:25 We're doing this, this is called McRoberts maneuver. 02:27 This opens up the pelvis, flattens out the sacrum and gives us more room in the posterior column so that you can put that anterior shoulder down to relieve that shoulder dystocia. 02:39 Next is provide suprapubic pressure. 02:42 Now this maneuver is performed not by the physician during the delivery but an assistant. 02:47 Whether that assistant be an obstetrician or a nurse, it's performed by someone else in the room. 02:52 As you can see here in this picture, what the assistant is doing is placing her hands in the CPR maneuver finding that anterior shoulder behind the pubic symphysis and rotating the shoulder forward. 03:05 That will relieve the shoulder's dystocia hopefully and get that anterior shoulders from behind the pubic symphysis. 03:14 Now, if our suprapubic and McRobert's maneuver have not worked, we want to start moving towards other maneuvers. 03:20 These maneuvers you can remember by saying, enter the vagina for internal rotation. 03:26 Now there's two internal rotations that we want to talk about here. 03:30 Woodscrew and Rubin maneuver. 03:32 So with the Woods' screw maneuver, you have two fingers behind the posterior shoulder. 03:37 Two fingers front of the anterior shoulder of the baby and you're rotating the baby to try to change the angle of the shoulder to relieve that shoulder dystocia. 03:47 Rubin maneuver is a little bit different. 03:50 You place two fingers behind the posterior shoulder to rotate the shoulder in. 03:55 You kind of folding the shoulders in like a taco decreasing the diameters between the shoulders to relieve that shoulder dystocia. 04:05 The next maneuver to consider is relieve the posterior arm. 04:08 Now, there is no literature to support which internal maneuver should be done first. 04:13 Meaning Woodscrew versus Rubin versus delivery of the posterior arm. 04:18 However, many practitioners to start with the delivery of posterior arm. 04:23 When you do that, this causes an increased space in the hollow of the sacrum allowing that anterior shoulder to be delivered downward. 04:31 Care must be taken however with this maneuver. 04:33 As there is an increased risk of fracture of the clavicle and the head of the humerus. 04:38 Fracture of the head of the humerus is particularly dangerous and that it can disrupt the blood flow to the humerus and cause necrosis of the joint. 04:47 And then one other maneuver we can try is rotate the patient to hands and knees. 04:53 This is known as Gaskin Maneuver. 04:55 And it's aim for a famous mid-wife Ina Gaskin. 04:58 What you do is you place your patient on hands/knees position. 05:01 So basically on our pores. 05:02 This rotates and changes the angle of the pelvis so that the baby can be delivered and that shoulder dystocia can be relieved. 05:10 Now the downside of this maneuver is that the patient has physically be able to roll over. 05:15 Remember the patient previously is on her back and now she needs to rotate hands and knees. 05:20 So this is not an option for our patients that have an epidural. 05:26 Now when you've done those other maneuvers and they haven't worked, we do have some additional maneuvers. 05:30 However, before you proceed to these additional maneuvers, you do want to try the maneuvers that we discussed a couple of times to see if you change the angle of the pelvis and that anterior shoulder enough that you can deliver that shoulder dystocia. 05:44 However, if you have done those a couple of times and you're still unable to relieve the shoulder dystocia. 05:48 Here's some additional more risky maneuvers that we can try. 05:52 First is breaking the clavicles. 05:54 So to break the clavicles of the fetus, you want to place your finger underneath the clavicle and pull out. 05:59 It's very important to pull out and not push in. 06:03 If you push in you can break the clavicle and clavicle can then puncture the lung. 06:07 You can break one clavicle or you can break two clavicles. 06:10 You can imagine that once the clavicles are broken, now your shoulder diameter is much shorter and you can deliver that shoulder dystocia--relieve that shoulder dystocia. 06:20 The next maneuver is Zavanelli maneuver. 06:22 This one is very tricky. 06:24 You basically have to take the infant and go through the cardinal movements of labor in reverse and push the baby into the uterus to then go perform a cesarean section. 06:32 This maneuver is very difficult to perform and should only be considered if you've done your other maneuvers and they have not been successful. 06:41 The next maneuver consider is a symphysiotomy. 06:43 With this maneuver you take a scalpel and you cut the cartilage that's in between the pubic symphysis. 06:50 Once you've done that, the shoulder will no longer be stuck behind the pubic symphysis. 06:54 Again this is a very risky maneuver and should only be done in a life or death situation when your other maneuvers have not been successful. 07:03 So the common complications of shoulder dystocia that we also need to discuss. 07:07 The first is brachial plexus injury. 07:09 Next clavicular fracture. 07:12 Then humerus fracture. 07:14 Asphyxia. 07:15 And then contusions and lacerations. 07:18 So let's talk about brachial plexus injury in some detail. 07:23 So with the brachial plexus injury, you can have either an Erb's palsy or you can have a Klumpe's palsy. 07:29 With Erb's palsy this is going to be injury to the C5 and C6 nerves. 07:35 And this comes from continuous downward traction on that neck when you have an anterior shoulder that is stuck and you're continually pulling down. 07:44 When you stretch those nerves, you can get an Erb's palsy. 07:47 Now these are often reversible with physical therapy sometimes surgery. 07:52 And with Erb's palsy that accounts for 75% of brachial plexus injuries. 08:00 Klumpke's comes from the injury to C8 and T1, again from that stretching of those nerves is not as common. 08:07 This only accounts for about 2% of lower nerve injury from brachial plexus. 08:12 And again this can be reversible with surgical intervention. 08:17 So let's take a case. 08:19 A 41 year old Gravida 2 Para 2 female just delivered a 5010 gram female infant. 08:26 The delivery was complicated by a shoulder dystocia requiring 4 maneuvers to deliver the shoulder dystocia. 08:33 You are called to the infant's bedside because the infant is not moving the left arm as much as the right arm. 08:40 What is the most common nerve injury responsible for this palsy? It is A. C5 and C6. 08:48 B. C6 and C7. 08:50 C. C7 and C8 or is it D. C8 and C9. 08:56 The answer is A. 08:57 C5 and C6. 08:59 Remember this is our Erb's palsy and this accounts for 75% of brachial plexus injuries.
About the Lecture
The lecture Labor Stage 2: Shoulder Dystocia by Veronica Gillispie, MD, MAS, FACOG is from the course Intrapartum Care. It contains the following chapters:
- Abnormal Labor – Shoulder Dystocia
- Shoulder Dystocia – HELPERR
- Common Complications of Shoulder Dystocia
Included Quiz Questions
Which of the following statements about shoulder dystocia is FALSE?
- Episiotomy can release the impacted shoulder and directly relieve a shoulder dystocia
- Shoulder dystocia is unpredictable and the delivering physician must always be prepared for it
- Shoulder dystocia is when the anterior shoulder of an infant is impacted behind the maternal pubic symphysis
- Appropriate shoulder dystocia management requires more than one delivering provider
- Maternal obesity is a risk factor for shoulder dystocia
A 34-year-old G1P0 with a history of gestational diabetes and a BMI of 32 has just delivered the head of her infant after 3 hours of pushing. The delivering physician notes that immediately after delivery of the head of the baby, the chin is retracted against the perineum. What is the most appropriate next step the physician should take?
- Call for help
- Apply fundal pressure
- Zavinalli's maneuver
- Symphysiotomy
- Apply vacuum to help downward traction of the head
A 30-year-old woman with gestational diabetes just delivered a 4700-gram infant boy after prolonged labor. You are performing the initial newborn examination when you notice the baby's left arm is rotated inward with the forearm extended and pronated and the baby is not moving it spontaneously like his right arm. What is the most likely injury?
- C5-C6 nerve damage due to over extension of the infant's neck during delivery
- C8-T1 nerve damage due to excessive downward pressure on the infants head during delivery
- C6-C7 nerve damage associated with clavicular fracture
- Humeral head fracture
- Intracranial hemorrhage due to protracted labor and operative vaginal delivery
You and your team have an emergency situation with a shoulder dystocia. So far you have tried McRobert's Position, adequate suprapubic pressure, internal rotation maneuvers, rotating the patient, and an episiotomy to try to reach in and relieve the posterior arm. Unfortunately, none of these maneuvers have worked so far, so you and your team decide the next best step to avoid further morbidity and mortality is to break the infant's clavicles to decrease width between the shoulders. What is the recommended method for breaking the clavicle?
- Place a finger under the clavicle and pull outward to avoid lung puncture
- Place a finger under the clavicle and pull outward to avoid brachial plexus injury
- Place a finger over the clavicle and push inward to avoid injury the vasculature in the neck
- You should never intentionally break the infant's clavicles
- Place a finger over the clavicle and push inward to avoid injury to the humeral head
Which of the following options best describes the appropriate method for applying suprapubic pressure?
- The assisting provider should stand on a stool at the side of the mother and place both heels of their hands above the maternal pubic bone and BEHIND the anterior shoulder of the infant and apply downward and forward pressure.
- The delivering physician should apply DOWNWARD pressure over the maternal pubic bone while keeping one hand ready to catch the baby.
- The assisting provider should apply downward pressure DIRECTLY over the paternal pubic bone.
- The assisting provider should stand on a stool at the side of the mother and place both heels of their hands above the maternal pubic bone and in FRONT the anterior shoulder of the infant and apply downward and forward pressure.
- The assisting provider should stand at the side of the mother and apply downward pressure over the anterior shoulder of the infant with one hand while applying caudal fundal pressure with the other hand.
Which of the following options describes the McRoberts maneuver?
- Lower the head of the bed and elevate the mother's legs while pulling them towards the chest to open up the pelvis
- Elevate the head of the bed and pull legs toward the chest to increase expulsive force in the pelvis
- Rotate the mom on hands and knees for delivery
- Insert 2 fingers behind the posterior shoulder and 2 fingers in front of the anterior shoulder and rotate the baby to a new angle
- Insert 2 fingers behind the posterior shoulder and fold the shoulder inward to decrease the width between the shoulders
A 34-year-old G2P1 with a BMI of 34 and gestational diabetes presented to the labor ward in active labor. She has a history of shoulder dystocia with her first delivery which was resolved with a few simple maneuvers. Her last baby was 4900 grams at birth, and she states this pregnancy feels slightly smaller than the last. She progressed through the first stage of labor rather quickly, but is now in a protracted second stage of labor after pushing for 3 hours with an epidural. Her cervical exam confirms complete dilation and unchanged +1 station since she started pushing. Should you perform a vacuum-assisted delivery at this time?
- No, this patient has multiple risk factors for a repeat shoulder dystocia. Cesarean section is the better option at this point.
- Yes, this patient has an arrest of the second stage of labor and should have an assisted vaginal delivery.
- No, this patient should be encouraged to continue pushing until there are signs of fetal intolerance of labor.
- Yes, even if she gets a shoulder dystocia, maneuvers can be done to undo it. Cesarean section should be avoided as much as possible.
- Cesarean section or vacuum-assisted delivery have equal risk in this situation and either would be the correct decision.
Which of the following is not a risk factor for shoulder dystocia?
- Advanced maternal age
- Maternal obesity
- Fetal macrosomia
- Gestational diabetes
- History of prior shoulder dystocia
Author of lecture Labor Stage 2: Shoulder Dystocia

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
As always, Dr. Gillispie has the best lectures. The treatment methods were explained very clearly.
