Playlist
Show Playlist
Hide Playlist
Serum Sickness in Children

-
Slides SerumSickness Pediatrics.pdf
-
Download Lecture Overview
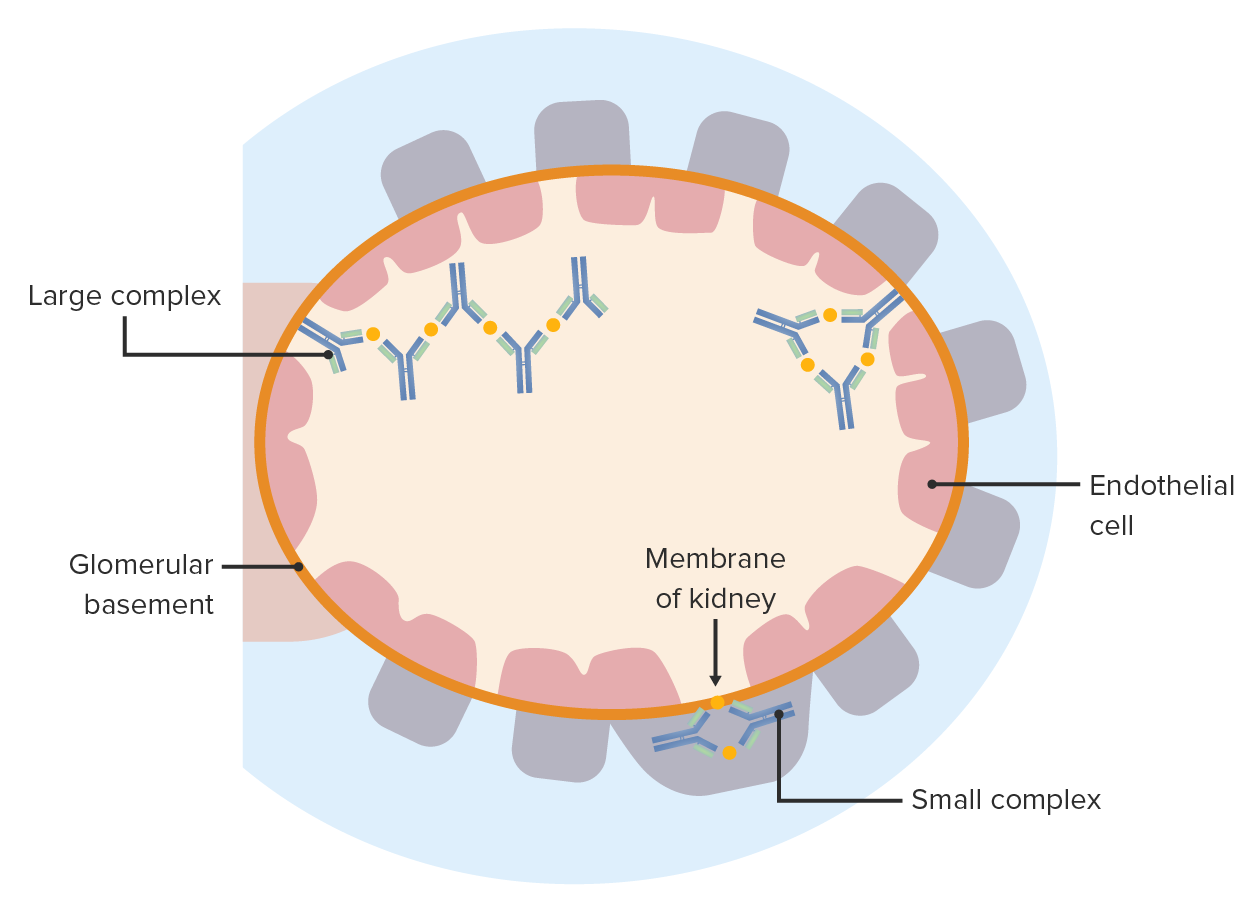
00:00 In this brief lecture, we will discuss Serum Sickness in Children. So serum sickness is a rare allergic disease that is a type 3 hypersensitivity reaction. I want to go through it in some details so we truly understand what it is. Basically, patients are administered a large amount of a foreign antigenic material. This can be either a medication or it can be classically antibodies. Individuals who receive antibodies from others or antibodies from other species are particularly prone to this problem and we'll talk about who gets antibodies from other species in a bit. Typically, this is an immune-mediated reaction between 1 and 3 weeks after your exposure. So patients will have a single large exposure to an antigen and then will break out with serum sickness. Alternatively, what can happen is certain individuals may get repeated or prolonged exposure to something and they may develop a chronic serum sickness that's less common and you have to be thoughtful about why is that patient continually being exposed. The most common cause in children is amoxicillin which interestingly is a large enough _____ that the immune system can respond to it in this way but this is different than in IgE-mediated response which is typically your allergic reaction to amoxicillin and it's certainly different than any other type of response such as the rash with amoxicillin and the Epstein-Barr virus which we talked about a little bit in the Epstein-Barr virus lecture. So what's classic with serum sickness is these 3 symptoms. Patients will usually have fever, they will have a diffuse erythematous rash and they will have arthralgia or joint pain. Typically, the rash can last between 1 and 14 days after the antigen is removed so we would stop obviously the amoxicillin, patients will gradually get better. Usually, the arthralgias follow the rash. So a patient first has the rash then starts developing joint pain and that's your clue but what makes this very different from other types of allergic reactions is the fever. These patients do have fever and you might be tempted to think this is an infection when in fact it's not. So this is something we have to clinically identify. Patients may have other symptoms as well. Those symptoms include CNS symptoms, perhaps facial swelling or facial tenderness and they can have nonspecific GI symptoms such as nausea, vomiting, or abdominal pain and that's typically from enteric edema. So, how does this happen? It starts off with the formation of immune complexes as a result of that molecule be it an antibody or amoxicillin or whatever the offending agent is. Then, there is a deposition of these immune complexes in tissues throughout the body and at those sites of deposition there is then inflammation and tissue injury. So here's an example of a patient who is having a serum sickness reaction. He is having a focal area where this rash is occurring and he's probably also having some joint pain. This patient was given antivenom. That's an example of an antibody from another species. It could also happen after IgG, for example, which is generally recombinant human antibody but in this case it was antivenom. Are all the antivenom was made out of horse serum? Now they make a recombinant sheep antibody for pit vipers that is a little bit less likely to cause serum sickness but it still concomitantly happen. So that's how this patient got affected. 04:13 Remember, children are much more likely to be bitten by snakes than adults are. About 10 days after he got the antivenom, he was doing better, he developed this fever, arthralgias and this rash which is classic for this problem. So how do we manage serum sickness? Well, we start off by removing the offending agent. Then we have to provide supportive care. Examples include NSAIDs for pain and fever and then also patients will have itching with the rash so we may provide diphenhydramine or some other oral antihistamine which provides some help with the itching. Generally, after you've had a serum sickness-like reaction you have to treat that as a true allergy. In other words, if a patient gets this from amoxicillin you really need to avoid amoxicillin for the rest of their life. So that's a brief summary of Serum Sickness in Children. 05:10 Thanks for your attention.
About the Lecture
The lecture Serum Sickness in Children by Brian Alverson, MD is from the course Pediatric Dermatology.
Included Quiz Questions
Which of the following constitute the classic triad of serum sickness?
- Fever, polyarthralgia, rash
- Fever, polyarthritis, oral lesions
- Arthritis, rash, oral lesions
- Fever, rash, confusion
- Fever, rash, bleeding
Which of the following is NOT true regarding serum sickness?
- Once rash appears, discontinuing the responsible agent has no effect on progression.
- It requires the presence of an antigen.
- It is immune mediated.
- It occurs 1-3 weeks after exposure to responsible agent.
- Most common triggering drugs are antibiotics.
Which of the following is a useful clinical feature in distinguishing serum sickness from Stevens-Johnson syndrome?
- Involvement of mucous membranes
- Skin rash
- Arthralgia
- Fever
- History of exposure
Author of lecture Serum Sickness in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture, I feel more confident to identify the disease and to differentiate it from other rashes.
