Playlist
Show Playlist
Hide Playlist
Septic Shock and Disseminated Intravascular Coagulation (DIC) – Thrombotic Disorders




-
Slides Bleeding Disorders and Thrombotic Disorders.pdf
-
Download Lecture Overview
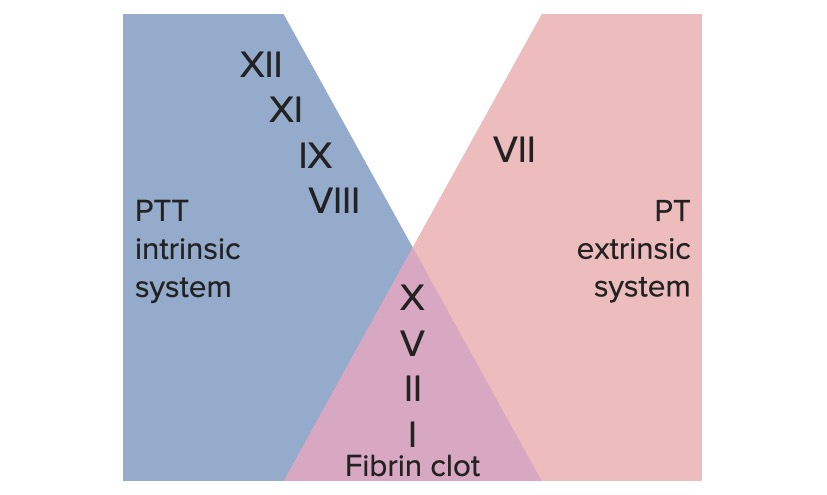
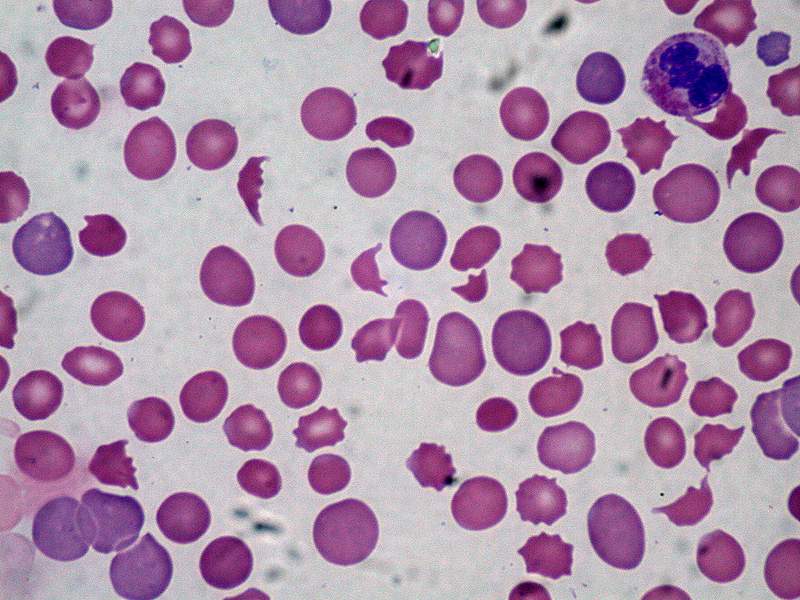
00:00 Let's talk for a moment about, "Septic shock" and the phenomena of “Disseminated Intravascular Coagulation” or “DIC.” So, sepsis, is all by itself a very pathologic state, will lead to very high degree of morbidity and mortality. 00:19 And septic shock is basically a response to pathogens, driven by the innate immune system and is caused by an overproduction of inflammatory cytokines. 00:31 These will have an effect on recruitment of inflammation throughout the body, the stickiness of various vascular beds and will cause extreme vasodilation, so, the patient goes into shock. 00:45 And clear-cut manifestation. 00:47 A predictable consequence of sepsis is, DIC or, “Disseminated Intravascular Coagulation.” If we think about it, in the site of a local infection, say, in your skin someplace, you would want to activate, many of the coagulation pathways, to prevent pathogens, from causing damage and causing bleeding. 01:13 So, in a localized environment, the activation that will lead to clotting makes sense. 01:21 But, if you have systemic activation, when there's only infection in one spot, then, you will get into a significant degree of morbidity and mortality driven by this, DIC phenomena. 01:33 So, let’s walk through, what's going on here. 01:36 On the upper part of this panel, you see bacteria. 01:38 Bacteria are releasing, “Pathogen-Associated Molecular Patterns,” or “PAMPS.” These stimulate cells of the immune system, of the innate immune system, macrophages, to produce cytokines. 01:51 You will also get, complement activation, you will get a number of inflammatory mediators, being released. 01:56 And again, if we keep it localized, to just where the bacteria are, that's a good thing, that's an appropriate response. 02:04 But, if we get too high a level, released systemically, then we start getting into issues related to activation of all these pro-inflammatory pathways and procoagulant pathways, everywhere, and that's when we get DIC. 02:20 So, here we have our pro-inflammatory mediators, that are being released into the bloodstream and they, at a sufficiently high level will act at a distance in other vascular beds. 02:30 One of the main effects besides, activating other inflammatory cells, is that, these pro-inflammatory mediators, things like tumour necrosis factor, interferon gamma, et cetera, will activate endothelial cells, in various vascular beds. 02:46 The endothelial cells, lining the vessels, will lead to vasodilation and increased vascular permeability. 02:54 Again, in a localized environment, that's exactly what we want to happen, however, if we do this systemically, that vasodilation, is going to cause hypotension and that increased permeability is going to cause us to lose fluid, in all tissues of the body leading to, edema. 03:11 So, that's one component of the activation of endothelial cells. 03:15 But when the endothelial cells are getting activated, other things are happening. 03:19 So, one, they will make more tissue factor. 03:23 That's what they should do, in an inflammatory setting, you want to make more things that are going to drive, pro-coagulation, so, you make tissue factor, which will, drive the extrinsic coagulation cascade, to make a thrombus. 03:35 We also, want to block the anticoagulation pathways, again, we want to drive coagulation in a localized setting, a good thing and systemic setting, not so good. 03:48 So, we're going to impair the anticoagulation pathways. 03:53 Things like, thrombomodulin, things like antithrombin III. 03:58 So we're going to impair those, the production of those and then we are also going to have the activation the production of plasminogen activator inhibitor. 04:11 Again, we want to make sure that, in a localized environment, we get the maximum prevention, against bleeding, but by doing this systemically we will engender, the formation of clots, everywhere. 04:24 So, those are things that the endothelial cells are making now, because they've been activated by the cytokines. 04:30 As a consequence, we will not be breaking down clots everywhere and we will be making more clots everywhere. 04:39 So, we will get increased fibrin deposition. 04:44 We will get, in that fibrin deposition, then the accumulation of platelets and we have platelet fibrin micro thrombi everywhere. 04:52 So, the systemic effects, of monocyte and macrophage cytokines, are that we will get, diffuse endothelial activation and thrombosis. 05:01 We will get more blood clots forming everywhere. 05:05 Things that we haven't talked about as part of sepsis, is that, we will also have reduced myocardial contractility, that will contribute to hypotension. 05:14 In addition to what's going on, because we have increased vascular permeability and we have vasodilation. 05:22 So, all these effects are going to contribute to sepsis, but the activation of the coagulation cascade, as we've talked about and the blockage or the inhibition of the anticoagulation pathways, will lead to disseminated intravascular coagulation. 05:39 With thrombosis and hypotension, you can imagine that you have multi-organ failure and as indicated there, the mortality even in the very best ICU’s around the world is 50%.
About the Lecture
The lecture Septic Shock and Disseminated Intravascular Coagulation (DIC) – Thrombotic Disorders by Richard Mitchell, MD, PhD is from the course Hemostasis.
Included Quiz Questions
Bacteria stimulate the release of what substance?
- Cytokines
- Fibrin
- Tissue factor
- Plasminogen
- Thromboplastin
Systemic activation of endothelial cells in DIC causes...
- ...vasodilation and increased permeability.
- ...the release of pro-inflammatory cytokines.
- ...platelet aggregation.
- ...prolonged PTT.
- ...deactivation of the complement system.
What is the mortality rate in patients with DIC?
- 50%
- 10%
- 25%
- 75%
- 30%
Author of lecture Septic Shock and Disseminated Intravascular Coagulation (DIC) – Thrombotic Disorders

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
