Playlist
Show Playlist
Hide Playlist
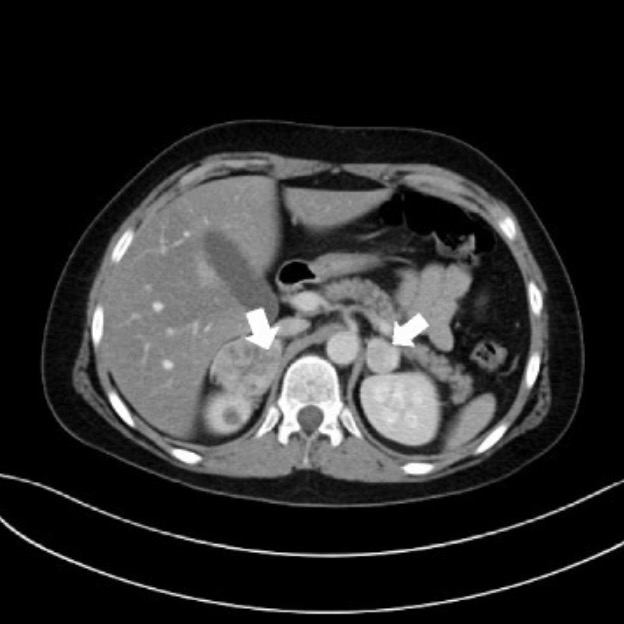
Renal Case: 47-year-old Woman with Palpitations

-
Slides Secondary Hypertension.pdf
-
Download Lecture Overview
00:01 Let's move on to another clinical case. 00:03 We have a 47-year-old woman in a previous state of good health. 00:06 She presents to the emergency department with palpitations, diaphoresis, headache, and this impending sense of doom. 00:13 She doesn't take any prescribed medications other than ibuprofen occasionally and doesn't take illicit drugs. 00:18 Her physical exams are remarkable for a blood pressure of 190/100 mmHg, per pulse rate is 130/min, noted to be in sinus rhythm, and she has a mild tremor noted on exam and pallor of her skin. 00:32 On screening labs in the emergency department, they're remarkable for a normal CBC and chemistry's negative urine drug screen. 00:40 Provided this woman's hypertension is due to a secondary cause, what would the most likely etiology be and what is our next step in establishing a diagnosis? Let's go through the case and see if we've got some clues here. 00:54 Now, our patient is complaining of palpitations, diaphoresis, this impending sense of doom, these are all symptoms of catecholamine excess. 01:02 She's got hypertension, she's tachycardic, she has a mild tremor on exam, and she's pallored. 01:07 Again, these can be signs seen in catecholamine excess. 01:10 Importantly on our labs, she has a negative urine drug screen so the likelihood of her having a stimulant use causing catecholamine excess is less likely. 01:21 So, taken together, what is the most likely etiology causing this woman's symptoms and what's our next step in establishing a diagnosis? Probably a pheochromocytoma. 01:33 And the next step that we wanna do in terms of clinching the diagnosis would be a 24-hour urine for fractionated metanephrines and catecholamines. 01:40 We'll go over this in the next couple of slides and you'll understand why.
About the Lecture
The lecture Renal Case: 47-year-old Woman with Palpitations by Amy Sussman, MD is from the course Secondary Hypertension.
Included Quiz Questions
What is the first step in the workup of suspected pheochromocytoma?
- 24-hour urine test for metanephrines and catecholamines
- A late-night salivary cortisol test
- Insulin-like growth factor levels
- CT of the abdomen
- Adrenal venous sampling
Author of lecture Renal Case: 47-year-old Woman with Palpitations

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
