Playlist
Show Playlist
Hide Playlist
Regional Anatomical Characteristics of the Vertebrae

-
Slides Regional Anatomical Characteristics of the Vertebrae.pdf
-
Download Lecture Overview
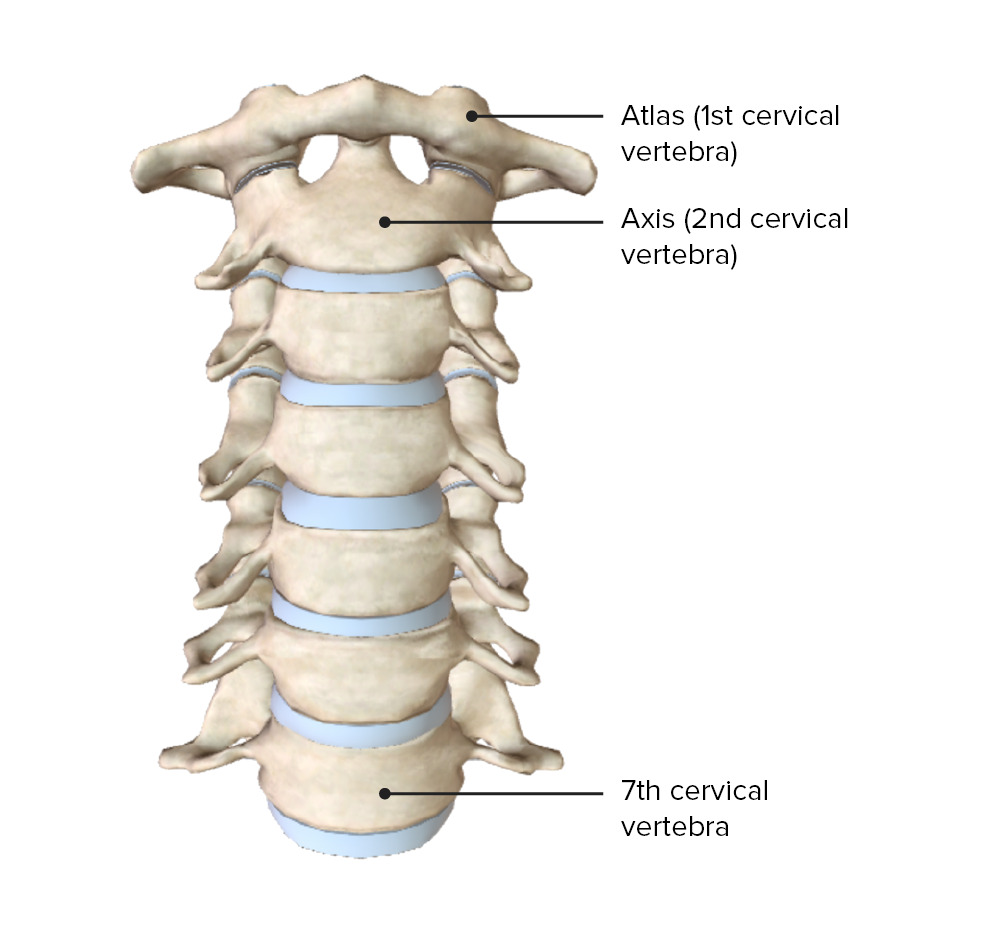
00:01 Now that we've seen the basic features of a vertebrae. 00:04 Let's look at some of the regional characteristics of vertebrae and how they differ from one part of the column to the next. 00:12 Let's start with the cervical vertebrae. 00:15 The C1 cervical vertebrae also goes by the name atlas. 00:19 Whereas the C2 also goes by the name axis. 00:24 C3, 4, 5, and 6, don't actually get a special name. 00:29 But then the last one C7 gets the name vertebra prominens because it has the most prominent spinous process. 00:39 Let's look at a typical cervical vertebrae. 00:43 So we still have a body that is somewhat square shaped. 00:47 And the superior surface is concave while the inferior is a little bit convex. 00:53 And from a superior point of view, we see that the vertebral foramen is a little bit triangular. 00:59 We have a feature we don't see in other transverse processes called the transverse foramen. 01:06 And several of the spinous processes are split or bifid. 01:14 Let's look at C1 or the atlas. 01:19 This looks very different from a typical vertebrae. 01:22 We have an anterior tubercle with an anterior arch, a lateral mass with the transverse process, and it's transverse foramen. 01:33 And then we have a facet for something called the occipital condyle. 01:38 And if you remember, occipital bone is the inferior portion of the skull. 01:44 So this is where the skull is going to rest. 01:46 And this is how atlas gets its name, because it's holding up the head essentially, sort of like Atlas was holding up the globe in Greek mythology. 01:56 And then posteriorly, we're connected by the posterior arch. 02:01 And we have a posterior tubercle, just like we have an anterior tubercle. 02:06 The next one down is also a very odd vertebrae, C2 or the axis. 02:13 Here we have an articular surface for the atlas above it. 02:17 But perhaps most unique feature is this process called the dens. 02:23 And as you can see, it's going to form a special type of joint with the atlas called the atlantoaxial joint. 02:31 And there's going to be rotation around this dens. 02:35 That rotation you can think of as sort of the motion when you shake your head no. 02:42 So let's look at the Atlantco-occipital joint. 02:45 So again, here we have C1 or the atlas. 02:49 And there are these bumps or condyles on the occipital bone that are going to interact with the articular surface on C1. 02:58 And they'll come together so that they can rest on the vertebral column here. 03:03 And there will be a nice degree of movement here, particularly in flexion/extension as if you are nodding your head yes. 03:13 Now, this is a very important connection. 03:15 So there's going to be a lot of very strong ligaments. 03:19 They combine the cranium and the vertebral column. 03:24 If we look down from the school's point of view, looking at the occipital bone, and its relationship to C1 and C2, we see that there's a ligament that actually goes around the dens and connecting it to the skull base called the alar ligament, as well as this criss crossing series of ligaments that have longitudinal portions, and transverse portions and they sort of form a cross hence the term cruciform. 03:51 And together all of these ligaments help limit the degree of rotation and flexion and extension so that we don't have damage to the passageway from our brain into our spinal cord here. 04:06 Similarly, this is the tectorial membrane we mentioned that is continuous with the posterior longitudinal ligament. 04:13 So it serves to strengthen the connection through the vertebral column up to the head. 04:19 Now let's look at the thoracic vertebrae, which we have 12. 04:24 Here the body is a little more heart shaped and the vertebral foramen is a little more circular. 04:31 And we have new features that we didn't have in the cervical vertebrae. 04:36 For example, we have these costal facets. 04:40 We see their inferior ones on the vertebrae above superior ones on the vertical below, and also ones on the transverse process called the transverse costal facets. And costal refers to rib. 04:54 So this is we're going to have the costovertebral joint with the head of the rib and tubercle of rib interacting with the vertebrae here, and these joints are synovial joints. 05:07 So we have a good degree of movement here. 05:10 We also have to have stability so we don't have too much movement. 05:13 So we have the costotransverse ligament. 05:18 We have the superior costotransverse ligament, and its lateral costotransverse ligament, all providing stability at this joint. 05:28 Now we're down to the lumbar vertebrae. 05:31 Where the bodies start to look cylindrical, and they're a bit bigger than they are elsewhere in the vertebral column. 05:36 The vertebral foramen is a little bit triangular again. 05:40 And we have a slight difference in our orientation of our articular facets. 05:46 The spinous process is also tend to be a little less prominent than say the cervical ones. 05:53 There's also some differences in the posterior spaces between vertebrae. 05:58 So if we were to look at the thoracic vertebrae, we see they're pretty small gaps here. 06:03 By the time we get down to the lumbar vertebrae, they're actually pretty big gaps. 06:08 And that's pretty helpful because this is also the area where we do lumbar punctures, and try to access cerebrospinal fluid. 06:19 Now we're down to the sacrum and coccyx. 06:23 The sacrum has an articular surface for the last lumbar vertebrae which will be L5. 06:31 And then it narrows down to a point at the apex where it's going to interact with the coccyx. 06:36 The anterior surface is very concave and there are these openings or anterior sacral foramina on this side. 06:46 Similarly, there are a convex surface on the posterior aspect. 06:51 And there are posterior sacral foramina. 06:54 And there's a passageway for the remnants basically of the vertebral foramen called the sacral canal. 07:02 And at the very inferior end the bones don't quite fuse all the way together to form something called the sacral hiatus. 07:10 And sometimes this can be a useful opening. 07:13 If you're going to provide a type of anesthetic block to the sacral area.
About the Lecture
The lecture Regional Anatomical Characteristics of the Vertebrae by Darren Salmi, MD, MS is from the course Back Anatomy.
Included Quiz Questions
Which vertebra is known as the atlas?
- C1
- C2
- C7
- T1
- T2
What is the shape of a cervical vertebral body?
- Square
- Rectangle
- Circle
- Octagon
- Triangle
Which of the following is NOT part of the lateral mass of a vertebral body?
- Anterior tubercle
- Transverse foramen
- Transverse process
- Articular facet
Which vertebra is known as the axis?
- C2
- C1
- C7
- T1
- T2
Author of lecture Regional Anatomical Characteristics of the Vertebrae

Darren Salmi, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
