Playlist
Show Playlist
Hide Playlist
Pneumonia and Pulmonary Infections: Etiology

-
Emergency Medicine Bord Pneumonia and Pulmonary Infections.pdf
-
Download Lecture Overview
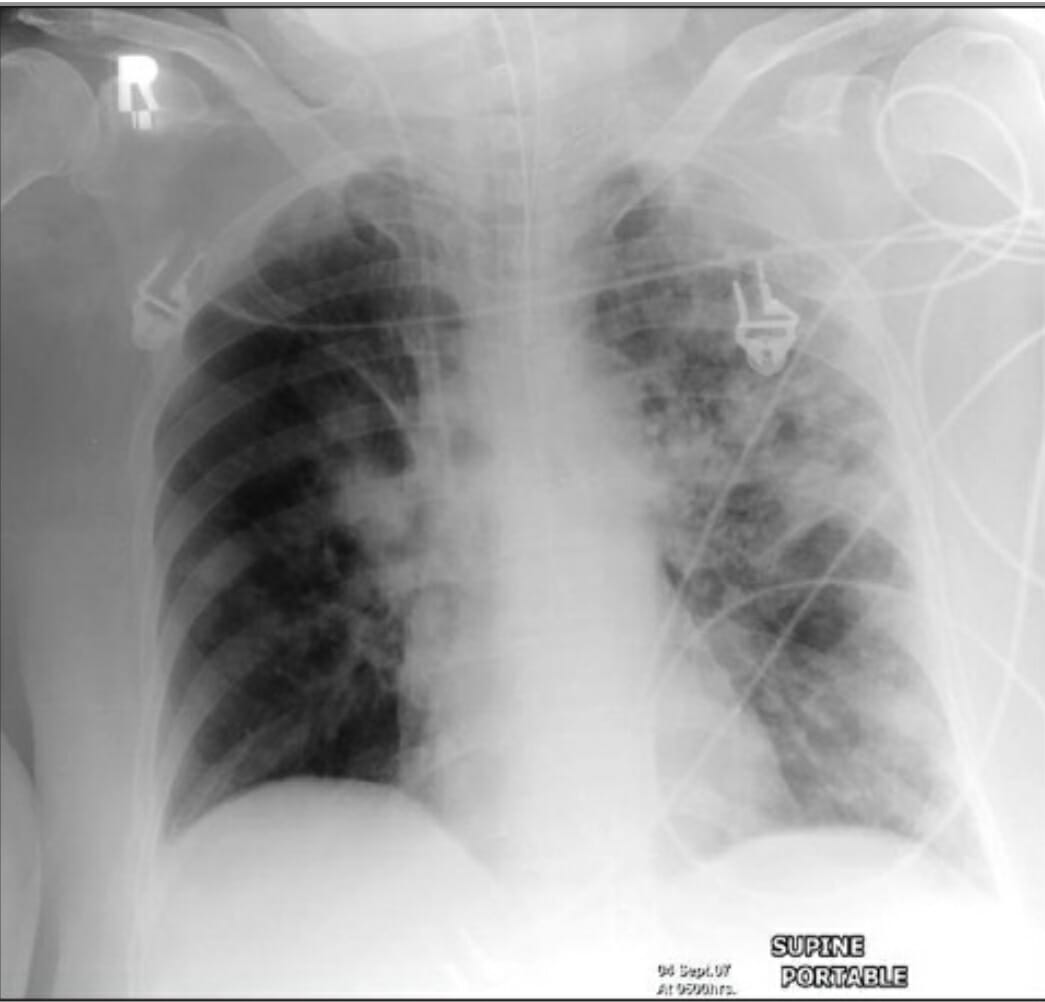
00:01 So what are our most likely and most common causes here for pneumonia? Streptococcal pneumoniae is definitely one of the most common causes, staph aureus, pseudomonas, especially you wanna think about that in patients who have recently been hospitalized and you wanna make sure you cover it for hospitalized patients when you’re selecting your antibiotics, Klebsiella pneumoniae, I’ll just take a moment to touch on this. 00:26 A Klebsiella classically presents with what they ask about on board exams as currant-jelly sputum, its a kind of a thick, nasty looking sputum, more common in patients who have a history of alcohol abuse, or homeless patients, it’s kind of the classic thinking. 00:43 Haemophilus influenzae, and then moraxella catarrhalis are kind of the most common bacterial pathogens that we think about. 00:52 Thinking about pneumococcal pneumonia, the highest risk for pneumococcal pneumonia are very young patients as well as the elderly, and those with a depressed immune system. 01:01 Definitely patients that have had a splenectomy are additionally at increased or higher risk for pneumococcal pneumonia, so you might wanna think about that when you’re thinking about what bacteria could be causing the infection. 01:16 The classic history for pneumococcal pneumonia is a sudden onset of fever, rigors which are shaking chills, so patients who describe to you that they have true and classic shaking chills that their whole body was shaking and they were very, very chilled, that is an indication that potentially pneumococcal pneumonia is present. 01:34 Patients who have shaking chills like that oftentimes do have a concerning infection, so keep that in mind. 01:39 This is one of those symptoms that may not seem super impressive or super exciting to people but really generally does make me a little bit worried, especially in the right clinical setting. 01:50 Bloody sputum, so does the patient cough and do you see blood in the sputum? Again, that’s an indication potentially for pneumococcal pneumonia, and does the patient have a cough? A very classic presentation symptom for pneumonia in general. 02:04 This is looking at a chest x-ray for pneumonia and this is a pretty classic picture of a lobar infiltrate. 02:11 So you can see at the base of the left lung that there is blurring of that hemi diaphragm. 02:16 You’re potentially not able to see the heart border very clearly and that area that’s more bright white is indicative of a lobar infiltrate. 02:25 Other lobar infiltrate patterns to kind of for you to be aware of would be a right middle lobe pneumonia which presents at an interesting way on a chest x-ray. 02:33 So on a film, basically, you would see blurring of the right heart border. 02:37 So that’s something for you to keep in mind when you’re thinking, could the patient have a right middle lobe infiltrate? Now, a staph aureus pneumonia is something that generally people are really sick when they come in with. 02:48 The onset is generally a little bit more gradual, so it’s a little bit less sudden than that pneumococcal pneumonia presentation. 02:56 Now, staph aureus can cause empyemas which are basically like an abscess in the lung or a multi-lobar infiltrate. 03:04 So instead of just one lobe of the lung being affected, it could be affected in multiple portions of the lung. 03:10 Now, pneumonia that occurs in the setting of viral illnesses such as influenza can actually lead to staph aureus pneumonia. 03:17 So if someone comes in and they’ve been sick for a period of time with influenza or influenza-like symptoms and then they go ahead and they become more sick or more ill after a period of maybe even being a little bit better, that should make you think about staph aureus. 03:31 So definitely consider it in that appropriate clinical setting. 03:34 Again, the reason that this is important is 'cause it can potentially affect the antibiotics that you give someone because not all antibiotics are effective against staph aureus. 03:45 Other kinds of bacteria that can cause pneumonia, legionella, and we’ll touch on that in a moment, chlamydia pneumonia is generally chlamydia psittaci and that is the one that can cause and lead to pneumonia. 03:59 Different than the one that causes a genital infection, and then mycoplasma is the other one. 04:04 Generally, we call these atypical because they present a different appearance on the lung x-ray. 04:09 So instead of it being a lobar infiltrate, what it will be is it will be more of a diffused infiltrative pattern, so all throughout the lung tissue, you’ll see that there’s abnormalities. 04:20 Viral pneumonia is classically caused by influenza as well as varicella. 04:25 So varicella for the most part, many people who are born nowadays are vaccinated against varicella, so don’t actually go through acute illness but it’s important to note that if you’re taking care of someone who hasn’t been vaccinated, this is one of those times in the ED that you wanna try and remember to ask about vaccination that that patient could potentially have varicella pneumonia, especially if they also have the classic rash associated with varicella or chicken pox. 04:53 Legionella pneumonia, most common in the summer months and that’s primarily due to a decrease in the other pathogens. 04:59 So most of the time, patients will get pneumococcal pneumonia or those lobar infiltrates more in the winter months or the times that it’s colder. 05:09 The infiltrates for legionella pneumonia are classically diffused and patchy rather than distinctly lobar and it’s commonly associated with GI symptoms. 05:17 So legionella pneumonia associated with diarrhea and vomiting, and possibly abdominal pain. 05:22 A little historical information, legionella pneumonia was first discovered at a legionnaire’s conference and historically, at least in that situation was associated with water sources, so it was due to the air-conditioning units having infected water, I believe. 05:38 So definitely in those situations, you wanna think about legionella. 05:42 So oftentimes, these might occur with like different groups of people or possibly related to a hospital acquired source. 05:49 So keep that in mind when you’re thinking about legionella pneumonia and especially the key things here are pneumonia with associated GI symptoms is kind of the classic presentation here. 06:01 Aspiration pneumonia is something else to consider and think about. 06:04 You wanna think about aspiration pneumonia in someone who potentially might not be able to protect their airway necessarily effectively or has had a period where they’re not able to protect their airway. 06:16 Patients who have had cardiac arrest or who have experienced a period of unconsciousness is kind of a classic thing. 06:22 Patients who are chronic alcohol users or drug users can have periods where they’re unresponsive where they may potentially also be vomiting or have aspiration of their gastric contents, so the portions of their stomach going into their lung tissue. 06:37 Now, aspiration may or may not be witnessed so always definitely keep it in mind that in someone who has an appropriate history or an appropriate kind of picture that may lead to that and the infiltrates for an aspiration pneumonia are most commonly in the dependent portions of the lungs. 06:53 Now, we always think of a right lower lobe infiltrate as being something that potentially developed due to aspiration because technically, from the lungs, that’s the most direct way to get into the lung tissue by the right lower lobe. 07:09 So thinking about aspiration being in the right lower lobe is one of the key things.
About the Lecture
The lecture Pneumonia and Pulmonary Infections: Etiology by Sharon Bord, MD is from the course Respiratory Emergencies.
Included Quiz Questions
What is the most likely etiology of pneumonia in an alcoholic patient presenting with currant-jelly sputum?
- Klebsiella pneumoniae
- Streptococcus pneumoniae
- Pseudomonas aeruginosa
- Haemophilius influenzae
- Staphylococcus aureus
What is the most likely etiology of pneumonia in an elderly patient with a history of splenectomy?
- Streptococcus pneumoniae
- Klebsiella pneumoniae
- Pseudomonas aeruginosa
- Haemophilius influenzae
- Staphylococcus aureus
What causes aspiration pneumonia to be more commonly observed in the right lower lobe?
- More vertical orientation of the right mainstem bronchus
- Weaker immune system of the right lung
- Narrower caliber of the right bronchus
- Increased aeration in the right lung
- Lack of goblet cells in the right bronchus
Author of lecture Pneumonia and Pulmonary Infections: Etiology

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
