Playlist
Show Playlist
Hide Playlist
Prostate Cancer Screening

-
Slides OtherCancerScreening PreventiveMedicine.pdf
-
Download Lecture Overview
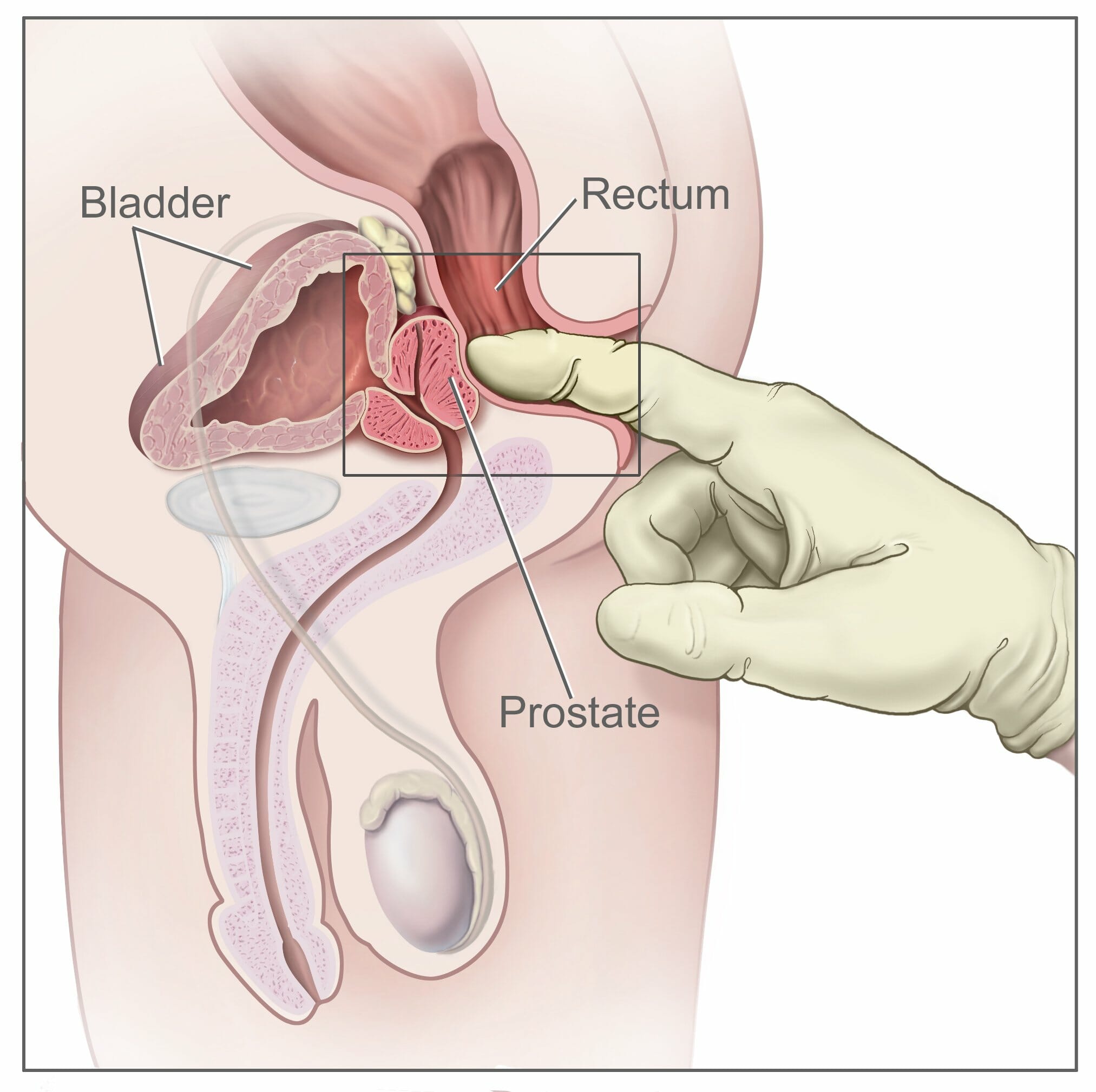
00:01 All right. 00:01 So we’ve spent a little time giving some focused attention on screening for breast cancer and screening for colorectal cancer, and now I’m going to cover screening for some other important forms of cancer, and just a hint, it’s prostate and lung. 00:15 All right, let’s get going. 00:16 Start with a case. 00:18 You have a 51-year-old asymptomatic man, no family history of prostate cancer. 00:23 He wants to know if he should be screened for prostate cancer. 00:26 What can you tell him regarding prostate cancer screening recommendations from the US Preventive Services Task Force? A. He should be screened with a digital rectal examination plus a prostate-specific antigen, or B. He should be screened with a PSA only, C. He should not be screened for prostate cancer, or D. There is insufficient evidence to recommend for or against prostate cancer screening? The answer is C. 00:52 He should not be screened for prostate cancer. 00:55 It’s easier to think about D because the Preventive Services Task Force is ambivalent because of a lack of evidence about a lot of different conditions, but they recommended against screening for prostate cancer due to a lack of certain benefit and some risk of harms. 01:13 So let’s look at the epidemiology of prostate cancer. 01:16 In terms of how common prostate cancer is, it certainly seems to meet the criteria for screening from that perspective. 01:23 The lifetime prevalence is nearly 17%, 60% of those tumors are diagnosed above age 65 years, and as you get older, 70% of prostate cancer deaths are found among men who are 70 years old or more. 01:43 However, that has to be counterbalanced by the overall risk of mortality. 01:48 Prostate cancer is associated with only 3% of all deaths among US men. 01:54 So despite those statistics of how common it is and how it tends to produce death among older men in particular, it’s a fairly low impact on overall male mortality. 02:08 And in fact, only about half of prostate cancers become symptomatic during a man’s lifetime. 02:14 The others never become symptomatic, and therefore, really don’t cause any kind of problems, and that’s the tricky part with prostate cancer. 02:23 Common and can be aggressive, yet also can be frequently indolent and, therefore, never really affect a man who’s already 84 years old who develops it for example. 02:34 So one thing I’ll advocate is is that the digital rectal examination really adds nothing, and they’ve done some research on this, adds nothing to PSA testing alone. 02:43 Patients hate it, and rarely it’s been associated with cases of moderate bleeding or even infection and sometimes severe infection that’s related to paraspinal abscess. 02:55 And so therefore, there are some risks with just doing the digital rectal examination besides just embarrassment alone, and in general, my rule is I don’t see much of an indication for doing the digital rectal examination at all among asymptomatic patients. 03:11 Very different if you’re having a lower urinary tract symptoms or rectal bright red blood, then, sure, but that’s a symptomatic patient. 03:20 Asymptomatic patients for screening purposes, I don’t do a DRE. 03:26 So what we do employ is generally a PSA testing. 03:29 And the most effective threshold for saying what’s normal versus abnormal is controversial. 03:35 The most common threshold is 4 mcg per liter. 03:39 Above 4 mcg per liter is considered suspicious or a positive test. 03:43 But that threshold is associated with a very high false-positive rate and it has a not insignificant false-negative rate. 03:51 You really want to see a very low, low false-negative rate with a screening test. 03:56 Now, what do we do when we get a positive PSA test? We refer to urology and they’re probably going to get transrectal ultrasound with biopsy assuming that this is asymptomatic average-risk patient. 04:09 So just understand that the PSA is associated with a higher rate of detection for prostate cancer once they do that testing, the relative finding of cancer is 63% higher versus no screening. 04:26 But up to a third of men experience some substantial side effects after a prostate biopsy. 04:32 So that prostate biopsy test is expensive, it’s uncomfortable, and is associated with bleeding and some other substantial side effects, which shouldn’t affect people in the long run, but it can certainly be uncomfortable around the time of the procedure. 04:49 So there are two major randomized trials of prostate cancer screening that are worth knowing. 04:54 One is the Prostate, Lung, Colorectal, and Ovarian Screening Trial, or PLCO Trial, that was done in the United States, enrolled 77,000 men between 55 and 74 years of age. 05:06 They found no difference in a screening group based on PSA versus a control group with no screening in terms of prostate cancer mortality. 05:15 Even though in the screening group, as predicted, they found more prostate cancer itself. 05:21 Limitation on this trial, the major limitation, is that there was significant contamination, over half of the group that was not supposed to get a PSA testing as part of the trial got PSA testing in their clinical practice. 05:34 And so, it was a negative trial that made PSA testing look ineffective, but they did have this significant limitation attached to it. 05:44 The European Randomized Study of Screening for Prostate Cancer was even larger, 160,000 men aged between 55 and 69 years of age. 05:52 They did find a statistically significant reduction of prostate cancer mortality with screening, and this is important because it’s the only major prospective trial to do so. 06:01 Yet the efficacy was only 1.28 reduced deaths per 1,000 men enrolled. 06:08 So the number needed to screen in this case was really high, 781 men needed to be screened to prevent one prostate cancer death. 06:17 And in fact, they also calculated that 27 cancers would have to be treated to prevent that one additional death as well. 06:25 So that’s a lot of time, a lot of money, a lot of morbidity and side effects when we think about cancer treatment in order to prevent that one cancer death. 06:36 So while there was a statistical significance in this trial, you know, how it plays out in terms of clinical significance and how it should play in the recommendations, that’s a pretty controversial area. 06:50 And yet we know that 90% of men with prostate cancer decide to undergo curative therapy. 06:56 And that therapy is highly effective for treating prostate cancer, but do recall, radical prostatectomy, which is one of the more popular choices still associated with rates of urinary incontinence of about 20% and erectile dysfunction in up to half, and those are significant impacts on quality of life. 07:14 Urinary incontinence really changes people and their habits. 07:18 I mean think about like going to movies, long car trips, everything becomes a risk, and therefore, patients can be really debilitated and depressed, who have urinary incontinence. 07:30 So there are some less invasive treatments as well. 07:33 What about external beam radiation therapy or implanted brachytherapy? Those are also effective, can be similarly effective and less invasive, but still some risks for chronic loose stools, for urethra stricture, still significant rates of erectile dysfunction. 07:52 So let’s look at recommendations. 07:54 The Preventive Services Task Force says that harms outweigh benefits and they recommend against. 07:59 The American Cancer Society, which is generally pro, pro cancer screening advocates shared decision-making for people at age 50 and for African-Americans beginning at age 45. 08:11 The American College of Physicians is a little bit discouraging, but recommends some form of shared decision-making as well. 08:18 And the time to do shared decision-making is before you order the PSA, by the way, because after you order the PSA and it comes back at 6, now you’re kind of obligated to recommend that the patient go see a urologist and get further testing for prostate cancer. 08:32 So it’s really a decision best made before they go to the lab. 08:38 American Urological Association recommends just shared decision-making between 55 and 69 years of age, and the American Academy of Family Physicians recommends against routine prostate cancer screening. 08:49 And again, this is for average-risk men, not men, say, with a family history of prostate cancer.
About the Lecture
The lecture Prostate Cancer Screening by Charles Vega, MD is from the course Preventive Medicine. It contains the following chapters:
- Screening for Other Forms of Cancer
- Digital Rectal Examination
- 2 Major Randomized Trials of Prostate Cancer Screening
- Curative Treatment
Included Quiz Questions
Which of the following statements regarding prostate cancer is LEAST ACCURATE?
- Digital rectal examination decreases prostatic specific antigen levels.
- Digital rectal examination has low sensitivity and specificity for detection of prostate cancer.
- A prostatic specific antigen level of 3 ng/mL is normal in a 60-year-old man.
- Prostate screening confers a small benefit for reducing prostate cancer mortality.
- Shared decision-making is encouraged for prostate screening.
Which of the following is the most appropriate screening test for prostate cancer?
- Prostate-specific antigen
- Digital rectal examination
- Rectal ultrasound
- Prostatic biopsy
- Prostate needle aspiration
Which population of men is at a higher risk for prostate cancer?
- Black
- Hispanic
- White
- Asian
- Middle Eastern
What is the most appropriate age for initiating discussion of screening for prostate cancer in men with an average risk?
- 50 years
- 40 years
- 60 years
- 65 years
- 70 years
What is the most appropriate age for initiating discussion of screening for prostate cancer in Black men?
- 45 years
- 50 years
- 55 years
- 65 years
- 70 years
Author of lecture Prostate Cancer Screening

Charles Vega, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
i found it concise and informative that allows me to waste less time going through the textbook.
