Playlist
Show Playlist
Hide Playlist
Primary Sclerosing Cholangitis with Case

-
Slides Gastroenterology 15 Billiary System Pt2 Cholestatic Diseases.pdf
-
Download Lecture Overview
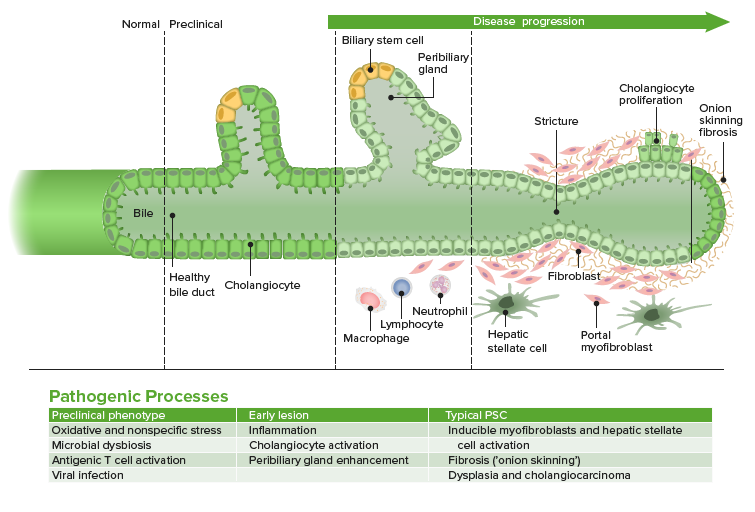
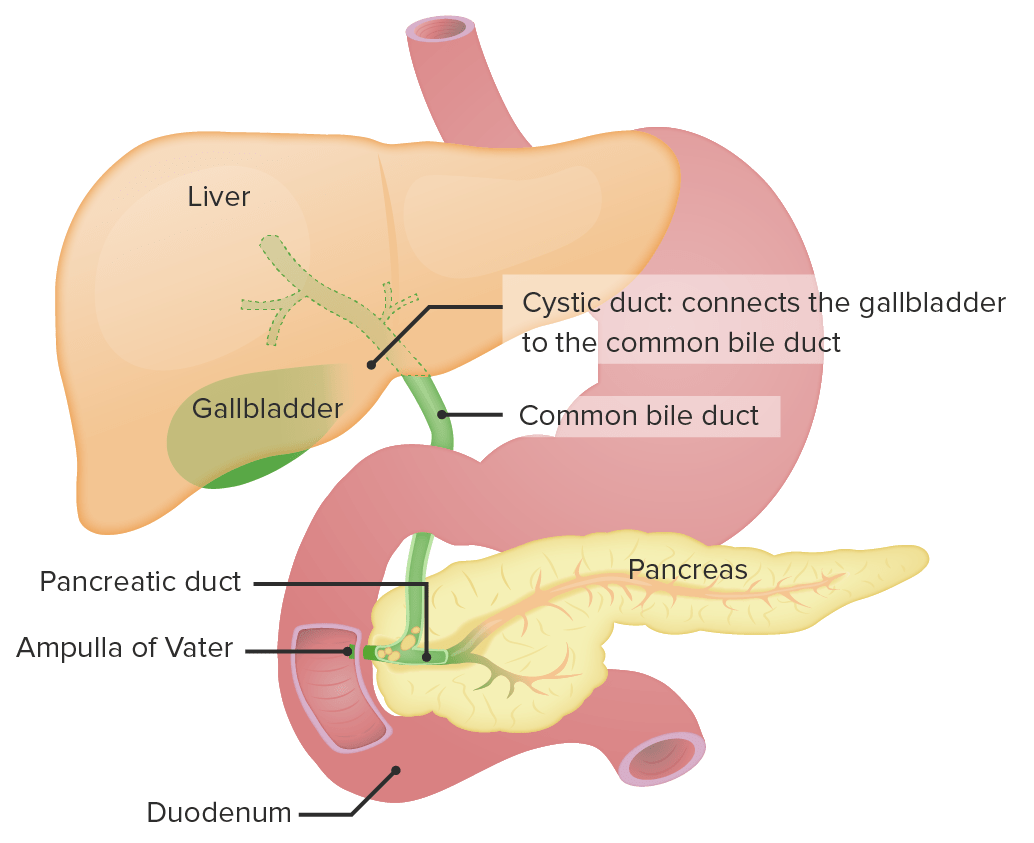
00:00 So now let's go on to our next case. 00:03 A 32-year-old man presents to clinic to follow up abnormal liver chemistry test. 00:09 His liver test we checked last month to evaluate a 3-month history of fatigue. 00:14 He has a history of diarrhea for the past nine months but has no known history of liver disease. 00:19 He has not had any abdominal pain, fever or jaundice. 00:23 Vitals are normal. 00:24 His exam reveals hepatomegaly but no splenomegaly. 00:29 There is no ascites, jaundice or spider angiomata. 00:33 Labs are notable for an AST of 92 (U/L), ALT 65 (U/L), alkaline phosphatase 475 (U/L) and total bilirubin of 1.4 (mg/dL) His abdominal ultrasound shows an enlarged liver with thickened extrahepatic bile duct but no intrahepatic biliary dilatation or masses. 00:53 So what is the best next step in diagnosis? Let's point out that he has a combination of fatigue, with abnormal liver test which should increase your suspicion for some type of hepatobiliary disease. 01:07 He does also have a history of chronic diarrhea which may be important a bit later. 01:13 In addition, on his physical exam and labs, he has hepatomegaly and a cholestatic pattern of elevation. 01:20 The ultrasound shows abnormal extrahepatic bile ducts but no other obvious abnormalities of the liver. 01:28 So that’s brings us to the diagnosis of primary sclerosing cholangitis or PSC. 01:33 This is an inflammatory disorder that affects the biliary system which can be either within or outside of the liver. 01:41 It tends to affect men more than women. 01:43 And will manifest with fatigue, a generalized pruritus and jaundice. 01:49 Both of these are caused by increased bilirubiin. 01:52 In addition, it can be associated with complications. 01:55 So the disease may progress and lead to cirrhosis, or scarring of the liver. 02:00 In addition, it is also associated with a high risk of cholangiocarcinoma. 02:05 It is also associated with many autoimmune diseases, in particular, ulcerative colitis. 02:12 And the diagnosis is made by looking for a cholestatic pattern of injury on your liver test, and performing an MRCP or ERCP to confirm the diagnosis. 02:24 Unfortunately for this condition, there is no really effective medical therapy. 02:30 What we can do instead is perform endoscopic dilatation of any strictures that are formed in the biliary system. 02:37 And when the disease becomes very severe, we can refer for liver transplantation. 02:44 So, we mentioned earlier that PSC has certain risks of different types of cancers. 02:49 It increases your risk of cholangiocarcinoma so patients who have this condition have a 10-15% risk in their lifetime of developing this type of cancer. 02:59 They are also at high risk for colon cancer, hepatocellular cancer if their disease progresses to cirrhosis and other types of gallbladder cancer. 03:11 So, earlier we mentioned that you could use an MRCP to make this diagnosis. 03:16 AN MRCP is magnetic resonance cholangiopancreatography Here on the left side you can see an example of normal common bile duct anatomy. 03:26 So you can see a normal common bile duct and normal hepatic ducts arising from it. 03:31 On the right side, this is an example of an MRCP showing the typical "beaded ducts" appearance of PSC so you see a very prominent and irregular looking common bile duct and irregular hepatic ducts as is seen in PSC. 03:47 So now we return to our case. 03:50 A 32- year-old man coming in with fatigue, known abnormal liver tests, chronic diarrhea which potentially raises your suspicion for inflammatory bowel disease such as ulcerative colitis and a cholestatic pattern of elevation with ultrasound showing abnormal extrahepatic bile ducts but no other obvious abnormalities. 04:11 So at this point, you should be suspecting PSC and the best next step to confirm the diagnosis is to do an MRCP or ERCP. 04:22 Thank you very much for your attention.
About the Lecture
The lecture Primary Sclerosing Cholangitis with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following is the diagnostic test of choice for primary sclerosing cholangitis?
- MRCP
- Abdominal CT
- Abdominal ultrasonography
- Endoscopic ultrasonography
- Colonoscopy
Which of the following is the treatment of choice for primary sclerosing cholangitis?
- Endoscopic dilatation of biliary strictures
- IV antibiotics
- IV fluids
- Elective cholecystectomy
- Proton pump inhibitors
Author of lecture Primary Sclerosing Cholangitis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
