Playlist
Show Playlist
Hide Playlist
Posterior Knee Dislocation

-
Slides Classic fractures Special Surgery.pdf
-
Download Lecture Overview
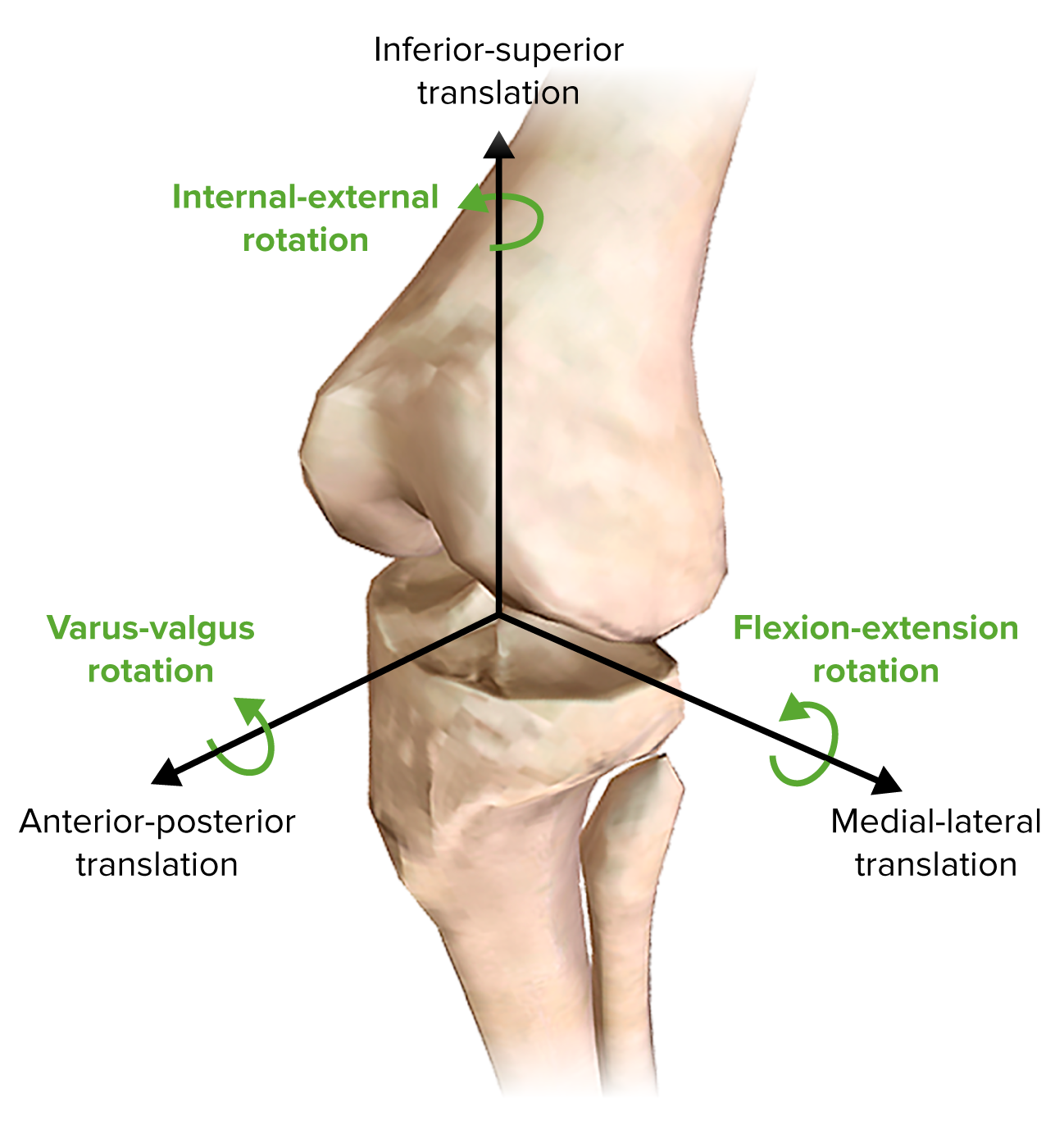
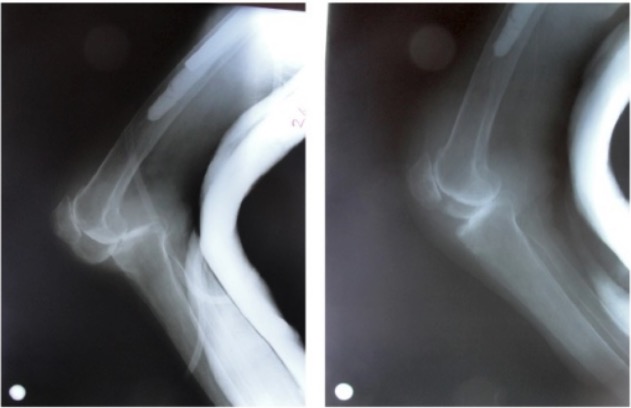
00:01 Now, let's move on to posterior knee dislocation. 00:05 This is an incredibly high-yield and important clinical entity. 00:10 Classically, it’s associated with a direct force to anterior knee in an anterior-posterior trajectory. 00:15 What’s the most common scenario for this? Just like this dummy in a vehicle. 00:20 The dashboard hits the knee causing a posterior knee dislocation. 00:27 On physical examination, there may be laxity of the ligaments holding our knee joint together. 00:32 There can be significant pain and sometimes obvious deformities, including a posterior dislocation. 00:41 Imaging shows a clear demonstration of a posterior dislocation on the right side of the screen. 00:48 You can see on physical examination on the left side of the screen that knee is incredibly edematous and swollen. 00:54 Additionally, you see an obvious deformity, likely a posterior dislocation. 01:00 And surgery is usually necessary in these situations. 01:04 Again, we like to reduce and immobilize. 01:08 These patients often have a knee immobilizer, so there's no actual flexion or extension of the knee, allowing the bones to heal as well as the ligaments. 01:17 Remember what are they at high risk for for periods of – long periods of immobilization? That's right. 01:24 DVTs and pulmonary embolism. 01:27 Let's now discuss popliteal artery injuries. 01:30 Popliteal artery injury is incredibly important to recognize and you should have a high index of suspicion whenever a patient has a posterior knee dislocation. 01:40 It’s so commonly associated with posterior knee dislocation that whenever I have a patient that have the dislocation, I always seek to make sure that the patient does not also have I always seek to make sure that the patient does not also have a concomitant popliteal artery injury. 01:53 Warm ischemia time is critical to limb salvage. 01:55 What does that mean? Warm ischemia time is the time where the tissues distal to the artery injury is not getting oxygen. 02:04 This is different than cold ischemia time, which is talked about in transplantation. 02:10 Cold ischemia time is when organs are preserved in solutions and put on ice. 02:15 The theory behind cold ischemia time is there may be a better chance of salvage if something is put on ice and the metabolism has been lowered. 02:25 You must suspect a patient of popliteal artery injury if there's a posterior knee dislocation. 02:32 Remember that mechanism of injury. 02:34 That dashboard on a head-on collision has intruded on to the patient and pushed the knee back with enough force. 02:42 Therefore, it's not difficult to imagine that the popliteal artery, as you can see on this image, can become injured. 02:49 Reducing the knee joint is the first step if distal pulses are absent. 02:53 Pulses normally return immediately post-reduction, but if they remain absent, urgent operative treatment may be required. 03:01 Now, let's revisit some important clinical pearls and high-yield information. 03:06 Remember, any significant fracture, particularly long bone fracture, demands evaluation of the associated vessels. 03:15 You should always consider the potential for vascular injury in these situations. 03:20 Now, let me ask you. 03:21 How would you assess for vascular injury in these patients? I’ll give you a second think about this. 03:28 That's right. 03:29 You feel the patient's pulses. 03:31 There is a caveat, however. 03:33 There’s an additional test called the ankle brachial index, particularly for the lower extremities. 03:38 We generally have a differential pressure between our ankle systolic blood pressure and our arm systolic blood pressure. 03:45 Any index less than 0.9 warrants additional vascular injury workup. 03:53 High-yield information for your examination. 03:55 Remember, fat embolism after long bone fracture is a classic association. 04:01 However, it’s difficult to diagnose. 04:03 Therefore, you must have a high index of suspicion. 04:06 Treatment, though, is largely supportive. 04:08 And again, the diagnosis depends on your index of suspicion. 04:13 Unfortunately, there's no confirmatory study for this. 04:17 I would recommend, however, that on a clinical scenario, with a patient having a long bone fracture and mental status changes and hypoxia, your answer choice should be fat embolism. 04:30 Thank you for joining me on this discussion of classic fractures.
About the Lecture
The lecture Posterior Knee Dislocation by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Posterior knee dislocations may occur as a result of which of the following forces?
- Direct force to the anterior knee in an anterior-posterior trajectory.
- An indirect force to the anterior knee in an anterior-posterior trajectory.
- Direct force to the anterior knee in an anterolateral trajectory.
- An indirect force to the anterior knee in an anterolateral trajectory.
- Indirect force to the anterior knee in a posterior-anterior trajectory.
How would you initially assess for potential vascular injury in patients with posterior knee dislocation?
- Ankle-brachial index test
- Angiography
- MRI
- Ct angiography
- Surgical exploration
Author of lecture Posterior Knee Dislocation

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
