Playlist
Show Playlist
Hide Playlist
Pituitary Tumors: Evaluation and Imaging

-
Strowd CNS Tumors Pituitary Adenoma.pdf
-
Download Lecture Overview
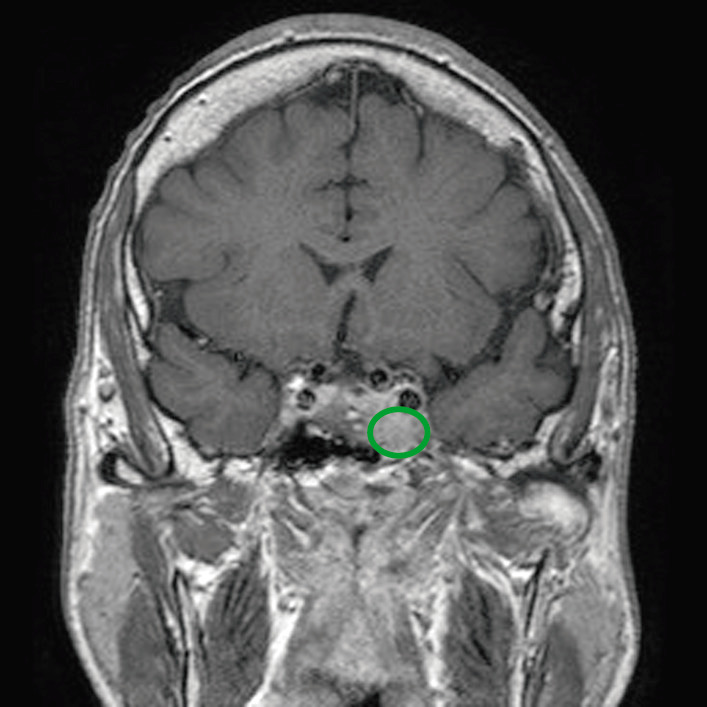
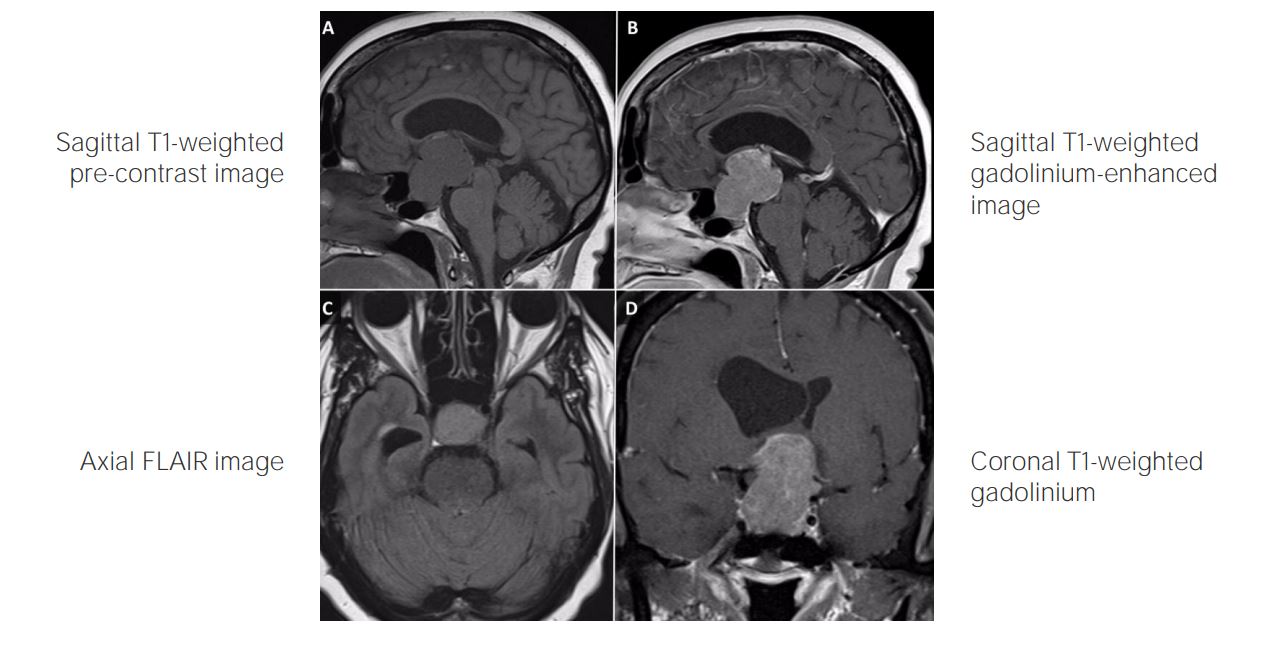
00:01 How do we evaluate these patients when we've recognized that a patient may be presenting with a pituitary lesion or a pituitary syndrome, what should we do? Well, the first is to image the patient. 00:12 And that's what was done in this case and we used an MRI. 00:15 MRI with and without gadolinium contrast to light up these tumors and with fine cuts through the sellar region is one of the most important initial steps in evaluating patients with suspected pituitary lesion. 00:29 Ophthalmologic evaluation is critical. 00:32 We said that the pituitary gland, the sella turcica lies in a close proximity to the optic chiasm, which sits just above this region. 00:41 In fact, the pituitary stalk goes right through the optic chiasm, and tumors that grow upwards, which is common can result in bitemporal hemianopia, which should be recognized either at presentation or followed with serial assessments after a lesion has been discovered. 00:58 And then hormonal evaluation is critical. 01:01 This is a tumor in and around the pituitary gland. 01:04 What is the pituitary do? It makes hormones. 01:07 Tumors that compress the pituitary can result in reduced hormone function. 01:12 And tumors that secrete hormone result in excess hormone secretion, and hormone function. 01:17 So we got to measure those things. 01:19 We need to look at prolactin, fasting morning cortisol, ACTH, growth hormone, insulin-like growth factor, TSH, and free thyroxine. 01:28 We get a lot of blood tests for these patients. 01:31 In selected cases, we also want to look at other pituitary hormone function like the gonadotropins, luteinizing and follicle stimulating hormone and maybe testosterone in patients where we suspect problems in those areas. 01:45 One important note for the imaging is that often the tumor enhances less avidly, less significantly than the normal pituitary gland. 01:56 And this is different than what we see with tumors in other areas of the body. 02:00 This can be very useful in determining the degree of displacement of the normal gland by the tumor. 02:06 An imaging may show right or left deviation of the gland or anterior posterior deviation of the gland, which can be important in our imaging assessment. 02:15 So these, the three things that really should be done for any patient presenting with a suspected pituitary lesion. 02:22 Let's take a closer look at a really substantial pituitary lesion, pituitary tumor. 02:28 We're gonna walk through the MRI imaging, For this patient, this patient presented with symptoms suggested of a pituitary lesion, headache and problems with vision of bitemporal hemianopia. 02:39 Here on the T1 image, this is a sagittal T1 image prior to contrast administration, we may or may not see a whole lot. 02:47 There is an extra mass, extra tissue in the middle of the brain. 02:50 And when we add contrast, it lights that tumor up. 02:53 And we see a large lesion that is beginning likely, beginning in the sella turcica right around the pituitary gland and expanding upwards in the area of the optic chiasm. 03:02 And this underscores the importance of optimal logic assessment in these patients. 03:07 On the axial imaging, we see a large circumferential circular lesion in the midline of the brain. 03:14 And on the coronal imaging again, we see that this lesion has expanded the sella turcica. 03:18 It looks bigger than the images we saw for our initial patient and this tumor is growing upwards, likely resulting in compression of CSF flow and hydrocephalus. 03:28 What's our differential for an image of that kind and a patient who presents with pituitary symptoms where we do imaging that shows this lesion, what could it be? Well, first we're going to think about a pituitary tumor because that's the most common cause of a lesion in this area. 03:43 And 90% are nonmalignant lesions that may not require a treatment. 03:48 The second is a craniopharyngioma. 03:51 These are histologically benign but often cystic epithelial tumors. 03:56 They show cysts on the imaging. 03:58 Instead of a large central homogeneously enhancing lesion, we see a small nodule with a cyst that often grows up into the brain. 04:07 Other lesions to know of but not focus on in significant detail, are the granular cell tumor of the sella, the pituicytoma, which is actually a glial based tumor located in the pituitary, which is kind of neat but very rare. 04:21 And the spindle cell oncocytoma. 04:23 Rare tumors that you may need to know of but not know about. 04:28 We also see non-neoplastic lesions occur in this area. 04:31 We see the Rathke cleft cyst, which is a cyst, it's not a tumor, and shows up as a cystic lesion, and can be confusing from a craniopharyngioma for an untrained eye. 04:42 And then rare lesions, xanthogranulomas, which are very rare and epidermoid cysts, which we talked about at the cerebellopontine angle. 04:51 So we think about both neoplastic and nonneoplastic tumors.
About the Lecture
The lecture Pituitary Tumors: Evaluation and Imaging by Roy Strowd, MD is from the course CNS Tumors.
Included Quiz Questions
Which of the following tumors is derived from remnants of Rathke's pouch?
- Craniopharyngioma
- Germinoma
- Prolactinoma
- Pituicytoma
- Granular cell tumor of the sella
Which of the following should be measured when assessing for acromegaly?
- Insulin-like growth factor-1
- Adrenocorticotropic hormone (ACTH)
- Prolactin
- Luteinizing hormone (LH)
- Fasting morning cortisol
Author of lecture Pituitary Tumors: Evaluation and Imaging

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
