Playlist
Show Playlist
Hide Playlist
Pediatric Pyloric Stenosis

-
Slides GD Pediatric GI.pdf
-
Download Lecture Overview
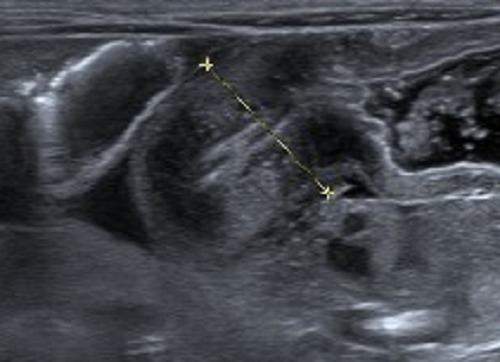
00:01 The topic is pyloric stenosis. 00:04 Before we move on, please understand where the pylorus is. Picture it. 00:09 You’re in the antrum of the stomach and you’re about to enter the first part of the duodenum. 00:13 What then happens here is the fact that the pylorus, which is a smooth muscle, technically it’s not even a sphincter, it’s a physiologic smooth muscle hypertrophy that may take place excessively resulting in gastric outlet obstruction. 00:32 So if there’s outlet obstruction, you can’t get into the duodenum what's the only direction that this chime can move in? Projectile vomiting. 00:42 And the vomit that you’re going to experience or see here is going to be non-bilious because you haven’t connected the common bile duct yet. 00:52 Risk factors: Males, and we’re not exactly sure why. 00:56 Usually first born, it’s interesting. 00:59 And the ratio of males to females is 4:1. 01:02 So boys, much, much, much more so. 01:04 Look for family history of pyloric stenosis. 01:08 Signs and symptoms: Non-bilious projectile vomiting, often after three weeks of age in that boy. 01:16 The “happy vomiter” is what they’re called and may have palpable olive in the right upper quadrant. 01:24 That’s where you’d expect your pyloric -- or hypertrophic pylorus to be. 01:28 The definitive diagnosis is usually made by Ultrasound and will show a thickend elongated pylorus. 01:34 Aditionally an upper GI-series can show a dilated stomach with an elongated pylorus and that is also a defended diagnostic method. 01:42 Here, supportive therapy is important. 01:44 Hypokalemia, hyperchloremic, metabolic alkalosis might be a possibility because of the vomiting. 01:52 Our management will be supportive. 01:55 Remember, with pyloric stenosis, you have a young boy who’s vomiting quite a bit. 01:58 So with that vomit, remember, this will be a metabolic alkalosis. 02:02 And with that vomiting taking place, you might be worried about potassium and, well, electrolyte disturbances. 02:10 Once the supportive therapy has stabilized the patient Ultimately surgical correction is necessary.
About the Lecture
The lecture Pediatric Pyloric Stenosis by Carlo Raj, MD is from the course Pediatric GI Pathology.
Included Quiz Questions
Which of the following causes pyloric stenosis?
- Hypertrophy
- Atrophy
- Hyperplasia
- Metaplasia
- Dysplasia
What is the examination finding seen in hypertrophic pyloric stenosis?
- Palpable, "olive-like" mass in the right upper quadrant
- Palpable, "sausage-like" mass in the umbilical region
- Doughy abdomen
- Board-like, rigid abdomen
- Cystic mass in the abdomen
A 1-month-old infant presents with non-bilious projectile vomiting for 2 weeks. The patient was diagnosed with pyloric stenosis. What is the anticipated electrolyte disturbance?
- Serum Cl – decreased, serum K – decreased
- Serum Cl – increased, serum K – increased
- Serum Cl – increased, serum K – decreased
- Serum Cl – decreased, serum K – increased
- Serum Cl – no change, serum K – decreased
Which of the following electrolyte disturbances is associated with pyloric stenosis?
- Metabolic alkalosis
- Metabolic acidosis
- Respiratory acidosis
- Respiratory alkalosis
- No change in the metabolic status
Which of the following is NOT part of the diagnosis and treatment plan in patients with pyloric stenosis?
- Barium enema
- Surgery
- Rehydration
- Electrolyte disturbance correction
- Ultrasound scan of the pyloric region
Author of lecture Pediatric Pyloric Stenosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
