Playlist
Show Playlist
Hide Playlist
Pediatric Pulmonary Embolism (PE)

-
Slides Pulmonary diseases in older children.pdf
-
Download Lecture Overview
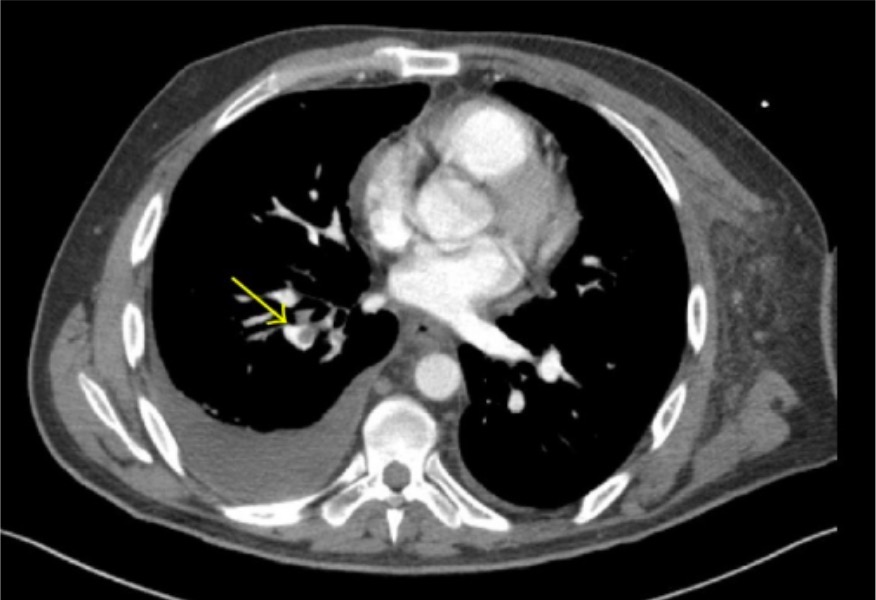
00:02 In this lecture, we’re going to discuss pulmonary diseases that show up in older children. 00:07 Now, we’re going to exclude cystic fibrosis, which has its own lecture, and we’re excluding pulmonary diseases that show up in infants, which also has its own lecture. 00:18 This is really other problems in children. 00:22 Let’s start off with pulmonary embolism. 00:26 So a pulmonary embolism can happen, but it’s very in children compared to adults. 00:34 It is seen more commonly in diseases or circumstances where there’s a predisposition to forming a clot and the mortality rate is only 20% that of adults. 00:48 In other words, children are more likely to have smaller pulmonary embolisms and they’re more likely to survive the event and live past it. 00:59 So in order to understand the pathophysiology of the pulmonary embolism, we have to recall Virchow’s Triad, the three things that are resulting in a clot inside a blood vessel. 01:11 One is stasis, one is the hypercoagulable state, and the other is endothelial damage. 01:18 And we have these three things, we’re at increased risk for creating a thrombus inside the child. 01:25 That thrombus can then proceed up and into the lungs, where it causes the pulmonary embolism. 01:32 One way to remember it is I's and O's. 01:35 So there are Is and Os that are responsible for causing pulmonary embolism. 01:40 The I's are indwelling central lines, prolonged immobilization, or inherited disorders of coagulation. 01:50 Remember, in kids, they present with unusual congenital problems more often than adults do, so these inherited disorders are something we will absolutely think of in a child who presents with a pulmonary embolism. 02:05 The O's: obesity, oral contraceptive pills, or orthopedic surgery, which is really more of the immobilization, but a nice way to remember that. 02:17 So in terms of the pathology of the disease, most pulmonary embolisms start as a thrombus in a vein, and then fly into the lungs. 02:27 This is usually starting off in a lower extremity but can be in the upper extremity, the pelvis, the kidney, or even just the right side of the heart. 02:36 And as we say it before, these are rare, but even rarer still are air emboli, tumor emboli, or fat emboli, which can cause similar symptoms, but aren’t necessarily from a clot. 02:50 So the pulmonary embolus, if it’s rare, how do we suspect it? These patients will typically have a history of sudden onset pleuritic chest pain. 03:03 They’ll have difficulty of breathing that is sudden onset. 03:07 About 50% of them will have a cough and about a third of them will have hemoptysis. 03:12 Hemoptysis in a child is never normal. 03:17 If they’re presenting with a massive pulmonary embolism, which is exceptionally rare and much rarer than in adults, these patients will have a sudden onset cyanosis and right ventricular failure. 03:31 These are the patients with jugular venous distention, hepatomegaly, they may have a single loud S2, other problems like that. 03:43 The majority of children presenting with a pulmonary embolism though are going to be non-massive PEs. 03:49 About half of these children will have tachypnea, they will often have tachycardia, and you may auscultate. 03:56 While you’re examining them, you may hear crackles, wheezing, or usually they’re just clear to auscultation. 04:05 So as you can see, a lot of these symptoms are somewhat nonspecific and in children it’s a rare condition, so you can imagine this is a challenging diagnosis to make, and it is. 04:17 One test that’s particularly helpful and important to know about is the D-dimer. 04:22 This is very important. 04:24 A positive D-dimer does not confirm a pulmonary embolism. 04:30 The D-dimer is an acute phase reactant that can be elevated by almost anything. 04:36 However, it’s almost unheard of to have a pulmonary embolism have a normal D-dimer. 04:43 So we routinely get the D-dimer as a way of ruling out pulmonary embolism. 04:48 If I have a patient with chest pain and tachypnea and I’m thinking maybe it’s a pulmonary embolism because the girl takes oral contraceptive pills, but I get a normal D-dimer, I usually won’t pursue this any further. 05:03 Other testing that’s important can be an ABG, which may show V/Q mismatch in the lung as a result of that clot. 05:11 A chest x-ray may show an area of collapse. 05:15 But, really, the most important test for truly ruling out a pulmonary embolism is the spiral CT. 05:22 Now, we do like to avoid radiation in children. 05:26 Remember, children are probably at more risk for cancer as a result of radiation exposure simply because there’s more mitosis going on and more opportunity for negatively impacting mitosis. 05:39 But the spiral CT is the way to go. 05:42 In the books, there will be mentions of V/Q scans; however, their accuracy at predicting pulmonary embolism is really no better than the spiral CT. 05:54 Also, you may read about angiography as the gold standard and this is absolutely true. 06:00 It is the gold standard, but really is very seldom used. 06:04 The reason being spiral CT is very good and angiography confers actually quite a bit of radiation.
About the Lecture
The lecture Pediatric Pulmonary Embolism (PE) by Brian Alverson, MD is from the course Pediatric Pulmonology.
Included Quiz Questions
Which test is most likely to rule out a pulmonary embolism in a pediatric patient?
- A normal D-dimer
- A normal arterial blood gas
- A normal chest x-ray
- A normal basic metabolic panel/CHEM-7
- A normal venous blood gas
A 16-year-old female comes to you with shortness of breath and chest pain. You suspect pulmonary embolism and proceed with necessary lab tests. Which of the following is a highly unlikely cause of pulmonary embolism?
- Isotretinoin
- Recent Immobilization
- Inherited coagulation disorder
- Obesity
- Oral contraceptive pills
Which of the following tests is used to rule in pulmonary embolism in a pediatric patient?
- Spiral CT
- ESR
- MRI chest
- Chest X-ray
- Arterial Blood Gases
Author of lecture Pediatric Pulmonary Embolism (PE)

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very good lecture. This allowed me to transfer my knowledge from the adult medicine to pediatrics regarding PE. However, I would have liked more info regarding the link with DVT and the clinical aspects of PE in children like clinical cases maybe and also a part about management. That being said I do understand it is not a typical pediatrics disease as it can be in adult medicine.
