Playlist
Show Playlist
Hide Playlist
Necrosis: Cellular Homicide

-
Slides Cellular Pathology Patterns of Injury and Cell Death.pdf
-
Download Lecture Overview
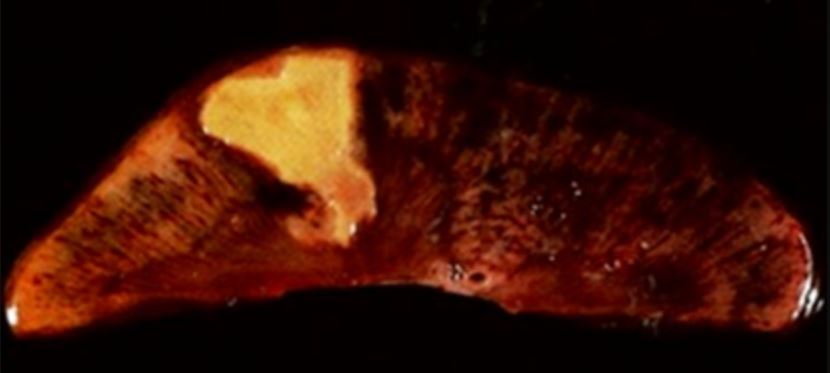
00:00 So when cells die by cellular homicide, there are two... 00:06 basic competing pathways. 00:08 One is that the proteins denatured. 00:10 They are still there. 00:12 They will eventually break down under the influence of inflammation. 00:15 But they're still there, and we can recognize the structure, that's coagulation necrosis. 00:20 So it's just denaturation the proteins. 00:23 And that's coagulation necrosis. 00:25 On the flip side is that we degrade it. 00:28 We have enzymatic digestion, and that's liquefactive necrosis. 00:32 It's still all dead, but depending on the tissue, depending on the length of time, etc., we may seem or less of one over the other, and we'll talk about that. 00:42 So those are the two basic flavors. 00:44 Coagulation necrosis, liquefactive necrosis, denaturation of proteins, enzymatic digestion. 00:50 We can also recognize cells is being eosinophilic. 00:53 So they get pinker on our typical hematoxylin and eosin stain. 00:59 And that's because we've lost a lot of the nucleic acids. 01:02 Nucleic acids, negatively charged things stained blue on the H and E hematoxylin and the eosin stain. 01:10 As cells die, that DNA and RNA and ribosomes, the things like that fragment and they don't pick up the hematoxylin and die. 01:18 So the cells look pinker because they're less blue. 01:23 They're also look pinker because denature proteins tend to pick up the ES and die more avidly. 01:28 So we can recognize that stuff because it's more eosinophilic. 01:32 It loves the pink better. 01:35 Also, we've mention that we have this influx of calcium, and that influx of calcium can bind and accumulate on negatively charged things like phospholipid. 01:46 So we may see calcium phosphate deposition as another marker of dead cells. 01:53 Mainly what we're going to see in terms of necrosis at the light microscopy level are these four elements. 02:03 So here's a good example. 02:04 This is myocardium and at the top, we have coagulated necrosis. 02:10 The tissue that's alive is at the bottom, and we can see that it's got a certain light pink color, and we see the material at the top is having a much more darker pink color. 02:21 That's the hypereosinophilia because we've lost all the nucleic acids and we stained better with ESN, and it's still though somewhat recognizable as cardiac myocytes. 02:35 And that's the denaturation process, the proteins of denatured in place. 02:40 So, denaturation of proteins, coagulation necrosis, enzymatic digestion, liquefaction necrosis will show you an example in a minute. 02:50 Hypereosinophilia and calcification, those are kind of the four elements that we've seen the light microscope. 02:55 There are also some characteristic nuclear changes in dead cells. 02:59 So we talked about chromatin, dissolving or chromatin falling apart. 03:05 Okay, there's some general changes that we need to also understand. 03:08 There's some characteristic nuclear changes. 03:11 On the top, we have your average hepatocyte. 03:15 With a nice, oval looking, normal sized nucleus. 03:20 As the nucleus, the nuclear material, the chromatin starts to degrade because of endonucleases, and proteases acting on it. 03:28 The nucleus can actually shrink. 03:30 It gets more condensed, it gets brighter blue, and that's called pyknosis. 03:37 You can also have complete fragmentation of that little pyknotic nucleus or the normal nucleus called karyorrhexis. 03:44 So you get little fragments of nuclear material kind of dispersed throughout the cell, that's karyorrhexis. 03:50 And then as we go further and further in the process, we break that down and it's not even recognizable as nuclear material anymore. 03:57 We've had endonucleases and proteases degrade everything that's going to stain blue and we get karyolysis. 04:03 So these patterns of nuclear fragmentation, pyknosis, karyorrhexis, karyolysis are also gonna be recognizable by light microscopy, as cells being dead. 04:15 This is just an example. 04:16 Again, this is in liver, and we have various arrows here. 04:20 So one we're seeing with the blue arrowheads, vacuolization. 04:26 These are just cells undergoing that cloudy swelling that edema. 04:30 So they have accumulating water and they look very swollen. 04:34 They're not yet dead, so those might be still alive. 04:38 And then we have pyknotic nuclei. 04:40 So in the middle of this image, you see rather large blue nuclei. 04:45 Now look up where the yellow arrowheads air pointing, those are little tiny condensed residual nuclei, those are pyknotic nuclei. 04:54 Where the chromatin is condensed, the nucleus has shrunk and that's all that's left. 04:57 That's a cell that's dying. 05:00 Then we have karyorrhexis. 05:02 And you can see the green arrow heads, representing areas of karyorrhexis altogether, where you can see little kind of stippling of the blue, that's fragmentation of the nucleus. 05:13 And then we have cells that have lost nuclear altogether, that would be the karyolysis and those are within the black circles. 05:20 So these are all the changes associated, nuclear changes with cell death. 05:26 So general patterns of necrosis. 05:28 We've talked about coagulated necrosis, which is basically denaturation and loss of nuclear staining. 05:36 And that's what this looks like. 05:37 So we have normal myocardial on the left. 05:40 You can see the nuclei, you can see everything. 05:42 And then on the right, in the right upper corner of the right hand side, where this coagulative necrosis those survival myocytes. 05:50 But in the middle, all the way across, hypereosinophilic and no nuclei in the cells, and that's coagulated necrosis of the myocardium. 06:01 Let's talk about contraction band necrosis. 06:03 This is a special form of necrosis that occurs in cells that are able to contract, so this is gonna be skeletal muscle. 06:11 This will be to some extent, in smooth muscle, but it's mostly in cardiac muscle, and what happens is cells have become ischemic. 06:19 They're no longer able to keep calcium out they get reperfused. 06:25 And now calcium that's in the blood in that reperfused environment comes screaming across into the myocyte. 06:34 When that happens, we will activate calpains and other things, of course, but that calcium is also a signal for this contract our cell to have the sarcomeres contract. 06:43 So we get these very hypertonic contractions. 06:47 It turns out that all you need for a muscle to contract is calcium. 06:50 It actually requires ATP for it to relax. 06:54 So when the cells are ischemic and dead, calcium comes in, they contract but they don't have any ATP, so they can't relax. 07:01 And we see these contraction bands. 07:04 Let's talk about liquefactive necrosis. 07:07 So liquefactive necrosis basically means there's no architecture left. 07:10 Enzymes have degraded everything. 07:14 So, you see around the periphery that we have normal liver parenchyma. 07:18 At the edges all the way around. 07:20 But in the middle, where asterisks gives, there's no architecture. 07:23 It doesn't look like anything. 07:25 It's all been dissolved, and that's liquefactive necrosis. 07:30 This happens very commonly when there are infections, bacterial infections in particular, and always in the brain. 07:37 We don't get coagulative necrosis in the brain. 07:40 For whatever reason, it's always liquefactive necrosis. 07:45 All right, let's talk about gangrene or gangrenous necrosis. 07:48 And there's nothing magical about these. 07:50 Once we've talked about coagulative necrosis and liquefactive necrosis. 07:54 We've pretty much covered the landscape, but there are three other terms at the bottom, that you need to be familiar with, because they will appear in the literature and you'll talk about them when you're on the wards and everything else. 08:05 So gangrene is really coagulative necrosis of an extremity. 08:11 And as it's typically used, if there is infection, meaning that there's going to be liquefactive necrosis, it's going to be wet necrosis, so there'll be a lot of liquefaction that's in there as well. 08:25 And if there is no infection, it's going to be dry, it's just going to be, coagulative necrosis and is just looking at gangrene. 08:32 That toe is dead. 08:34 And if we did a histology of that, it would be mostly coagulative necrosis. 08:38 At the base of the toe, there's a superimposed infection, and we'd see liquefaction. 08:44 Caseous necrosis, so caseous necrosis is classically characteristically associated with tuberculosis. 08:52 So when we talk about caseous necrosis, we're saying TB in another form. 08:57 Caseous? What does caseous mean? Caseous actually means cheesy for the Latin scholars out there, and it looks cheesy not through the microscope, but grossly, Grossly. 09:09 Grossly, it looks like cheese. 09:11 It looks like cottage cheese, but microscopically, we have zones of necrosis with lots of inflammation, and it's basically, it's basically liquefactive necrosis. 09:23 But there's a higher calcium content in this because of the bacteria, and we have a lot more necrosis in a central area with surrounding inflammation. 09:32 And that's where we get cheesy. 09:33 But it's basically liquefactive necrosis, of a different flavor. 09:38 And if we say caseous necrosis, we are talking about, in most cases, tuberculosis. 09:44 And finally, fat necrosis. 09:46 And fat necrosis occurs when there is activation of enzymatic activity that can break down lipid, and it gives us kind of an amorphous look to it overall. 09:58 So this is an example where there's fat necrosis in an infection in a breast tissue, which has got a fair amount of fat within it. 10:08 When that happens, the inflammatory cells that come in will degrade the fat and they break it down into little lobules. 10:17 Those little lobules actually have charge on them and calcium combined to them. 10:21 And we can actually get calcium soaps that form as a result of the calcium, that's in the tissues, interacting with the lipid that has been broken down from all of the adipocytes. 10:34 And we get this kind of gumesh. 10:38 It is just a variety of different sorts of necrotic debris. 10:43 So it's a variation truly on the liquefactive necrosis spectrum. 10:48 So let's fat necrosis. 10:49 So you will hear about each of these. 10:51 But in essence, everything is either coagulative or liquefactive necrosis or some combination. 10:59 And with that, we've kind of discovered and discussed the morphology of death.
About the Lecture
The lecture Necrosis: Cellular Homicide by Richard Mitchell, MD, PhD is from the course Cellular Injury.
Included Quiz Questions
Which of the following characterizes coagulative necrosis?
- Protein denaturation
- Pus formation
- Enzymatic degradation
- Activation of the coagulation cascade
- Hydropic degeneration
Which of the following is a hallmark of necrosis?
- Nuclear fragmentation
- Mitochondrial swelling
- Blebbing of the cell membrane
- Accumulation of fat vacuoles
- Basophilic cytoplasm
Which of the following is involved in the formation of contraction bands in myocardial infarction?
- Calcium reperfusion
- Increased ATP production
- Calcium release into the lumen of the sarcoplasmic reticulum
- Collagen and fibrin deposition
- Breakage of the actin-myosin bridges
Which of the following is most commonly associated with liquefactive necrosis?
- Brain infarcts
- Myocardial infarcts
- Acute pancreatitis
- Hypertensive emergency
- Tuberculosis
Which of the following characterizes fat necrosis?
- Formation of calcium soaps
- Fibrin deposition
- Cheese-like appearance
- Amyloid deposition
- Fat vacuoles accumulation
Which of the following is responsible for converting dry gangrene to wet gangrene?
- Infection
- Ischemia
- Calcium deposition
- Immune-complex deposition
- Radiation
Author of lecture Necrosis: Cellular Homicide

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great clarity, illustrations, and attention to detail. Thank you very much!
