Playlist
Show Playlist
Hide Playlist
Meckel Diverticulum

-
Slides GIP Meckel Diverticulum.pdf
-
Download Lecture Overview
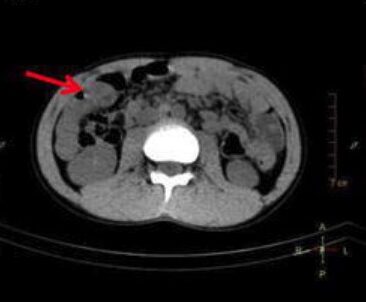
00:00 Welcome. We're going to have a nice, little short talk about a very cute entity. 00:06 And then, at the end of this, remind me and I'll tell you a story about how I will never forget about Meckel's diverticulum. 00:13 So, what is this? It is a developmental anomaly. It's not really even a defect. 00:21 It's a persistent remnant of the omphalomesenteric duct. We'll see how this forms in a minute and it's a true diverticulum. 00:28 It's all three layers of the bowel are present and what you're seeing is a little outpouching near the bottom that's in kind of red highlighted with green. Okay. That's a Meckel's diverticulum. 00:39 So, it's a cute little thing. The epidemiology. So, it turns out although, it's not all that common. 00:45 It's the most common congenital gastrointestinal tract anomaly. 00:49 And again, not really a pathology. It's just a developmental variation. The prevalence is about 2% of the population. 00:58 Although, the vast majority of patients are never diagnosed with this. They never know that they have it. 01:03 Males have it more frequently than females, about a two to one ratio. 01:08 And if symptoms are going to occur, they tend to occur relatively early on. 01:14 If you get past the age of two to four and you've not ever had anything associated with your Meckel's, it's very unlikely you'll have anything the rest of your life. 01:23 So, here are the rule of two's and this is a favorite medical school kind of mnemonic. 01:29 So, 2% of the population. These are typically found about two feet, so, 60 to 100 centimeters proximal to the ileocecal valve, so, it's in the distal ileum, about two feet away from the cecum. They're about two inches long. 01:43 They have two types of ectopic tissue, they have gastric and pancreatic. Those are the most common kinds. 01:49 Two years is the most common age of clinical presentation, a two to one male to female ratio. 01:54 So, you can remember the rule of two's. The pathophysiology of this. So, as they say, this is a developmental anomaly. 02:03 The normal yolk sac very early on in development is connected to the nascent primitive gut. 02:12 And it's connected via the vitellointestinal duct. 02:16 It also has mesenteric vessels within it. That connects the midgut to the yolk sac in utero. 02:23 Now, normally, the omphalomesenteric duct completely involutes, becomes a little fibrous nubbin, somewhere between the fifth and sixth weeks of gestation. 02:33 The baby no longer needs anything from the yolk sac, getting the entire nutritional blood supply from the mom's placenta through the umbilical arteries and veins. 02:42 So, there's usually that total involution. And then, you have a little umbilicus with the little fibrous indentation and the bowel completely inside. 02:52 That's the normal thing that happens in 98% of us. 02:55 However, in some cases, the proximal part of the omphalomesenteric duct fails to obliterate, leading to the small outpouching that we call Meckel diverticulum and then, pulls it out into a little diverticulum, all three bowel layers. 03:06 The clinical presentation. So, again, 98% of the time, totally asymptomatic. 03:11 If you're going to have symptoms, it's going to be usually lower GI bleeding, so, there is focal erosion or focal inflammation that gives local GI bleeding. 03:20 There may be some nausea and vomiting if there's small bowel obstruction. 03:24 So, this can be a way to get traction on the bowel and to get intussusception. 03:30 And part of that will be also abdominal pain and distention. Meckel's diverticulum, in the same way that the appendix has an outpouching and can have a proximal obstruction, you get the same thing happening in Meckel's. 03:43 So, that will lead to Meckel's diverticulitis. Obstruction proximally, expansion of bacteria distally, dilation of that part of the bowel, compromise the blood supply, inflammation. 03:58 Also, remember that there are a couple different ectopic tissues that can be found within a Meckel's diverticulum. 04:03 You can find gastric epithelium. You can find pancreatic epithelium. 04:07 And these can either get inflammation classically associated with either of those. 04:13 So, you can get peptic ulcers or pancreatitis or you can have the production of gastrin which will cause gastric ulcers up in the stomach. How do we make the diagnosis? Well, in the vast majority of patients, we don't - it's found incidentally. 04:29 It's found imaging for some other reason. Endoscopy, if we happen to have gone all the way via colonoscopy, past the cecum, into the proximal 100 centimeters or so of the ileum, we might find it, but it's not usually how it's found. It's usually found as an incidental diverticulum seen on CT, coming off that segment of bowel. The management. If you happen to have a Meckel's diverticulum and it's found incidentally on imaging, nothing to be done. It's just like, "You are so cool. 05:04 You're on of the 2%." On the other hand, if the patient is symptomatic, if there is fever, if there is pain, if there is bleeding, we're going to do the things that we would always do with any inflammation involving the bowel. 05:18 Make sure we give that patient hydration, put the bowel to rest, so, we're not allowing anything to be eaten. 05:23 Transfusions as necessary, antibiotics for impending perforation, and then, call your favorite surgeon if that needs to be resected. 05:31 The cute little story that has to be told about Meckel's diverticulum. 05:35 I was a medical student, I was in the operating room. I was with a surgeon who was notorious for yelling at everybody. 05:41 We were doing, I believe, an appendectomy, an open appendectomy back in the olden days before we did - before we did endoscopic appendectomies. 05:51 Anyway, he opens up and there is this thing sticking out of kind of the mid-ileum and he get - I could see that he was smiling behind his mask because he knew the medical student wouldn't know what it was. 06:04 And he turned to me and he said, "So, worm." No, he just said, "So, what is that?" And I said, "Well, I believe that's a Meckel's diverticulum." And I knew some of the things to say about it. 06:17 He goes, "All right. You may stay in my operating room." And I got an excellent evaluation for the entire rotation. So, remember that. Meckel's diverticulum. All right. Thanks.
About the Lecture
The lecture Meckel Diverticulum by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
Which of the following describes a Meckel diverticulum?
- Persistent remnant of the omphalomesenteric duct
- False diverticulum
- Persistent remnant of the allantois
- False diverticulum involving the umbilicus
- True diverticulum involving the umbilicus
Which statement about Meckel diverticulum is true?
- It affects 2% of the population.
- It is more common in women.
- It is found 2 feet from the rectum.
- It commonly presents at age 30.
- It is found 2 feet from the esophagus.
At what gestational age does the omphalomesenteric duct involute?
- 5th week of gestation
- 15th week of gestation
- 25th week of gestation
- 10th week of gestation
- 2nd week of gestation
Author of lecture Meckel Diverticulum

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
