Playlist
Show Playlist
Hide Playlist
Mechanical and Neurological Causes of Wrist Pain

-
Slides Osteopathic Considerations of the Wrist and Hand.pdf
-
Download Lecture Overview
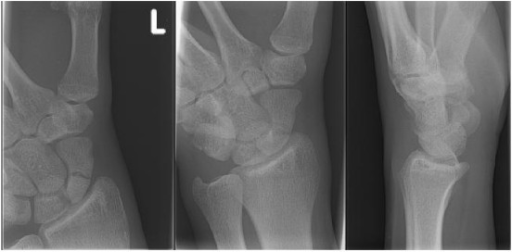
00:01 There are many different causes for wrist pain so in our differential, we have to think of a potential mechanical causes of wrist pain Fractures could be a potential mechanical cause, avascular necrosis, ligamentous tears, DeQuervain's tenosynovitis, potential neoplasms or ganglions and somatic dysfunctions are all possible mechanical causes of wrist pain. 00:23 Keinbock's disease is due to decreased blood flow to some of the bones in the wrist and then so that could develop into avascular necrosis of the lunate bone, you could have irritation and inflammation of your tendons and specifically if you have inflammation of the extensor pollicis brevis and ABductor pollicis longus, these tendons extend the thumb and so overuse injuries of the thumb could potentially contribute to DeQuervain's tenosynovitis is when you have pain along your thumb and in your metacarpal joints and so overuse sometimes could lead to DeQuervain's tenosynovitis. 01:09 There could be ligamentous injuries in the wrist usually due to trauma and so one of the relationships that you want to take a look at is between the scaphoid and lunate bone, sometimes on x-ray you'll see increased space between those bones leading to increase your suspicion for possible ligamentous injuries. 01:30 Patients with scapholunate ruptures tend to have more of a radial deviation of wrist pain whereas patients with lunotriquetral rupture of the ligaments tend to have more ulnar deviations of the wrist and increased wrist pain. 01:47 There are different orthopedic test that we could perform to help narrow down our differential, especially for suspicious of a specific injury and so if we are suspicious of a potential ligamentous injury between a scaphoid and lunate bone, we could perform a Watson's test. 02:04 What the Watson's test does is to check for the stability between the scaphoid and lunate bone, what we wanna do is to hold on to the scaphoid bone, and then we're going to start with the pateint's wrist in ulnar deviation and while holding pressure on that scaphoid, we're gonna have the patient try to radially deviate the hand. 02:26 As the patient moves her hand through the radial deviation, if the patient have any increased pain, then that would be a positive test or a positive Watson's test which indicates possible ligamentous injury between the lunate and scaphoid bone. 02:43 This is important to perform because if you have a missed scaphoid fracture, sometimes that could lead to avascular necrosis of the bone and there is severe injury. 02:56 Shuck's test is a special test we could perform to check fo perilunate instability. 03:01 So that lunate bone in the center of the wrist sometimes is suspect to injury and so if we wanna check whether or not the ligaments around that lunate bone has been injured, we could perform the Shuck test. 03:13 To perform the Shuck's test, what we do is we start with the patient's hand in flexion and while holding the patient's hand in flexion, we're gonna ask the patient to try to extend their wrist and as they extend their wrist, if there's pain in that area around the llunate bone, then that is a positive test indicating possible perilunate instability. 03:35 Finklestein's test is a test that we could do to check for DeQuervain's tenosynovitis and so remember DeQuervain's tenosynovitis is inflammation by the thumb so if the patient has a lot of pain by the thumb and the radial aspect of the wrist, we could perform this test. 03:53 The test is performed by asking the patient to hold their fingers around the thumb and then ulnar deviate their wrist. 04:00 This puts a stretch into those tendons and if there's inflammation, then there'll be acute pain there, so a positive test would be pain on the lateral wrist as the ulnar deviate, their fist with their thumb enclose within their fingers, so again a positive test indicates possible DeQuervain's tenosynovitis. 04:22 There are different neurologic causes of wrist pain. 04:25 we need to consider possible distal posterior interosseous nerve syndrome, carpal tunnel syndrome, injury to the radial nerve, injury to the ulnar nerve at the the tunnel of Guyon, or also thoracic outlet syndrome Carpal tunnel syndrome is due to compression of median nerve. 04:45 The median nerve runs through this carpal tunnel at the wrist. 04:48 The carpal tunnel's composed of the wrist bones, and also the flexor retinaculum on top of it. 04:55 Within this tunnel in the space runs our finger flexors and the median nerve and due to swelling or any sort of injury in this area, it could compress on that nerve and cause symptoms of decreased sensation and also atrophy of the thenar muscles and so what we could do is to perform different special test. 05:18 If we're suspicious of patients with numbness and tingling, usually more pain at night, decreased grip strength, we could perform two different tests to try to confirm carpal tunnel syndrome and so we have Tinel's test and Phalen's test. 05:36 Tinel's test is a test that we could perform along any nerve at different regions. 05:42 Tinel's sign itself for the median nerve is to check for the irritation of the median nerve as it passes through the carpal tunnel. 05:52 So here what we want to do is to tap along the carpal ligament along where the median nerve would run and just that tapping over that region, could reproduce that numbness and tingling and paresthesia over the median nerve distribution, that would be a positive test for carpal tunnel syndrome. 06:14 Phalen's test is another test that we could perform to check for carpal tunnel syndrome. 06:19 Here, we're gonna ask our patients to hold their wrist in flexion with the back of the hands together up for one minute, patients usually will complain of any sort of numbness and tingling and pain along that median nerve distribution that would indicate a positive test, and what you're doing here is because you're compressing along the wrist here that's gonna recreate the pain, An alternative to Phalen's test is a Prayer's test, and here you're gonna actually tell the patient to put the palms together kind of like holding your hands in prayer and that extension of the wrist is gonna irritate the nerve and again, numbness and tingling and pain would be a positive test. 07:06 Ulnar nerve compression. 07:08 So the ulnar nerve when it's compressed, will lead to increased flexion in the fingers and so because the ulnar nerve innervates the extensor tendons, the fingers will then be stuck more in flexion or give you this kind of claw hand deformity The ulnar nerve could be potentiallly compressed at Guyon's canal. 07:33 So Guyon's canal is where the pisiform and the hamate meet and along there is a small canal where the nerve passes through and innervates the pinky and the ulnar half of the forefinger, and so patients with numbness and tingling of the pinky and decreased grip strength especially of those fingers, you have your increased suspicion of ulnar nerve compression. 08:04 The ulnar nerve can also be compressed at the elbow. 08:07 So cubital tunnel syndrome occurs when the ulnar nerve is compressed as it passes by the medial epicondyle of the elbow. 08:17 And so this is similar to when you hit your elbow and they call it, "hitting the funny bone" and you get that shooting, radiating paresthesia into your fingers again more by the ulnar half of the forefinger and your fifth digit and so the ulnar nerve could be compressed at the cubital tunnel and patients could also have some decrease in grip strength. 08:46 Radial nerve damage, The radial nerve does not run through tight spaces like the ulnar and median nerve does so it does not tend to be entrapped like those two nerves, but the radial nerve can get injured due to acute trauma, injury, fractures and so if we injure the radial nerve, patients will have the inability to really extend the digits and also the wrist, you could also have a loss of sensation on the radial side of the hand The radial nerve divides and there's a posterior interosseous nerve that drops deeper by the elbow, and sometimes the posterior interosseous nerve could be entrapped and that will lead to weaknes of the wrist on extension but because it dos not do sensation to the hand, the sensation will be intact So if you have someone that has difficulty with extending the wrist and fingers, you have to suspect more of a posterior interosseous nerve entrapment especially if sensation is intact, There are many different systemic causes of wrist pain that we have to consider, patients with different metabilic conditions such as diabetes and hypothyroidism could have issues with the wrist and hand, patients with osteomyelitis, patients with rheumatologic disorders frequently present with wrist and hand complaints especially osteoarthritis, so with osteoarthritis, with wear and tear, there might be more pain with overuse, you might see more of the joints at the metacarpal joints, more inflamed and irritated with rheumatologic like rheumatoid arthritis, you'll see some nodules that occur along the fingers, sometimes, a lot of wrist pain, sometimes more deviations of the wrist and fingers. 10:40 Reflex sympathetic dystrophy usually secondary to some sort of trauma to the extremities and then patients will have uncontrolled pain, pain to just light touch, maybe dysautonomia to the hand, so there are lot of different things that could occur post trauma, usually after surgery or some sort of traumatic injury to cause reflex sympathetic dystrophy. 11:06 Peripheral neuropathy is also another potential systemic cause of wrist and hand pain that we need to consider. 11:15 Allen's test is a special test that we could perform to determine whether or not the blood flow to the hand, through the radial and ulnar artery is patent and intact, and so what we want to do with this test is to have the patient open and close your fist while we occlude the arteries and then release one at a time, and then when you release it, by occluding it have the patient pump their hand open and close the hands become more pale and then what you do is when you release one artery at a time, you should see that the hand starts to return circulation and become more pink and flushed, and so, you'd want to do that one side at a time, release one artery at a time to make sure it's patent on both sides and this is important to perform prior to any sort of arterial blood draws to make sure that there's proper flow from both sides and that you're not going to cause a clot or occlude circulation to the hand. 12:13 And so by understanding the anatomy and physiology of the hand and how to apply these different special tests, it could help us with better evaluating our patients with wrist and hand complaints and pain.
About the Lecture
The lecture Mechanical and Neurological Causes of Wrist Pain by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Wrist Region.
Author of lecture Mechanical and Neurological Causes of Wrist Pain

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
