Playlist
Show Playlist
Hide Playlist
Lymphocytosis – White Blood Cell Pathology

-
Slides Quantitative Disorders.pdf
-
Download Lecture Overview
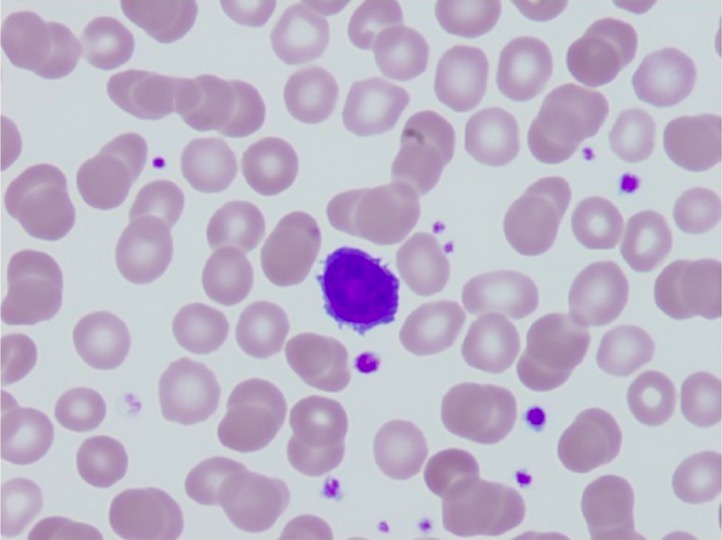
00:02 Lymphocytosis. 00:03 In the previous discussion, we looked at neutrophilic leucocytosis in great detail. 00:08 Let’s go ahead now and take a look at what causes lymphocytosis. 00:13 Elevated WBC count, yes, that’s where you begin and now, you have an absolute lymphocyte count greater than 4000 in adults or in a child, even higher 8000. 00:22 What is your normal WBC count? Good, 4500 to 11,000. 00:28 If you can remember some of these individual lymphocytes. 00:33 What kind of infection causes more lymphocytosis? Viral or bacterial, especially viral, but could also be bacterial. 00:41 I give you Bordetella Pertussis, chronic inflammation. 00:44 What does that mean to you? At some point in time, the neutrophils did not disappear or undergo apoptosis, they are being replaced by macrophages and lymphocytes and drugs. 00:57 Notice, as an example, I did not put corticosteroids. 01:02 Corticosteroids would cause lymphopenia. 01:04 You must memorize that, if you haven’t already. 01:07 The drug that I had given you example would be anticonvulsive therapy and Phenytoin. 01:13 With lymphocytosis, increased production might be a possibility or decreased entry into a lymph node, welcome to Bordetella Pertussis, which is a bacteria. 01:23 In either case, it finds lymphocytosis. 01:29 Antigenic stimulation of T-cells causes them to take an atypical morphologic change, if we are talking about EBV and remember, in infectious mononucleosis referring to Epstein Barr virus and I will show you a picture coming up and the-and the picture will be a lymphocyte which looks atypical. 01:49 Opt-Often times it is the nucleus, think about the nucleus of a lymphocyte, what does it look like? A sphere, sometimes a pathology recall an atypical lymphocyte that is found in EBV or CMV as a ballerina skirt, you will see what I am referring to. 02:07 Heterophile antibodies in acute phase is known as a monospot test, very, very sensitive. 02:11 This is what you will be using in the United States for-for your practice, especially in adolescence. 02:17 If this comes back to be negative, you could be pretty darn sure that your patient now is mono free and if you want absolute confirmation then you are called… what is something called the Epstein Barr virus nucleic acid type of issue, but this takes months, you don’t have this kind of time. 02:34 You see that? It takes months. 02:36 You, as a clinician, you want something fast and effective, then you are going to use the monospot test, but if you want confirmation, EBNA, it might be a possible-possible test here. 02:47 Remember, you are worried about splenic rupture in this patient. 02:53 In addition to EBV, viral hepatitis, cytomegalovirus, toxoplasma may result in this particular type of morphology that I will take a look at-that you will take a look at and it is called an atypical lymphocyte, I also call a Downey cell. 03:07 You know it as being a Downey cell, don’t you? Let’s go ahead and take a look at that atypical lymphocyte. 03:14 Take a look at these cells here, these are lymphocytes, they do not look normal whatsoever. 03:20 It is imperative that you don’t go back and take a look at what normal is, I have shown you one. 03:26 The nucleus of a lymphocyte, which you are seeing here dark purple, normally should be perfectly spherical, just about and then nucleus of a lymphocyte should be the size of the surrounding RBCs. 03:39 First off, this doesn’t even look like a sphere and second off, you can’t even compare it to the size of the RBC. 03:46 You find lots of cytoplasm and the one in the middle maybe, if it is typical text book, it is called what is known as a ballerina skirt. 03:54 If you see it, so be it; if you don’t, whatever, let it go. 03:58 It is just a description, they are not going to put it in a stem, but as pathologists, we do. 04:02 The point is these are atypical lymphocytes. 04:05 When would you find this? Viral infection. 04:07 Examples, please. 04:09 EBV being a big one. 04:11 Do not forget about CMV, toxo and maybe perhaps viral hepatitis. 04:16 Here, we will continue taking a look at leucocytosis. 04:21 Here, the increase in WBC count was caused by eosinophils. 04:28 Welcome to eosinophilia. 04:31 Allergies, asthma and also helminth infection will cause eosinophilia causing a rise in your WBC count. 04:41 From the granule of the eosinophil, especially parasitic infection, you are going to be releasing major basic protein so that you can try to kill off the parasite. 04:51 Basophilia, whenever you think about basophilia, for the most part remember, this is at the basement of the hierarchy of your WBC, at a measly 0.3 percent. 05:02 Hmm! If you find your WBC count to be elevated and it is due to a basophil, make sure you know what a picture looks like. 05:10 What does a granule look like by the way in a basophil? Oh, excuse me, apart from what it looks like, what does it contain? It is a very, very dark and it contains histamine. 05:18 One of the major myeloproliferative disorders that may contribute to basophilia is chronic myelogenous leukemia. 05:27 Monocytosis, chronic inflammation EBV, TB, Salmonella, many, many, many organisms. 05:32 Our topic here is leucopenia. 05:35 Let’s begin by looking at corticosteroids. 05:39 Corticosteroids may bring about lymphopenia due to apoptosis of B and T cells. 05:44 Eosinopenia may also occur, once again, apoptosis.
About the Lecture
The lecture Lymphocytosis – White Blood Cell Pathology by Carlo Raj, MD is from the course Quantitative White Blood Cell Disorders – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following is caused by corticosteroids?
- Lymphopenia
- Anemia
- Thrombocytopenia
- Polycythemia
- Leukemia
Which of the following drugs causes lymphocytosis?
- Phenytoin
- Dexamethasone
- Budesonide
- Methylprednisolone
- Prednisolone
Which of the following diseases is the Monospot test very sensitive to?
- Infectious mononucleosis (EBV)
- Syphilis
- Tuberculosis
- Gonorrhea
- Rubella
Which of the following are seen in infectious mononucleosis?
- Downey cells
- Burr cells
- Bite cells
- Popcorn cells
- Basket cells
Author of lecture Lymphocytosis – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
