Playlist
Show Playlist
Hide Playlist
Long Thoracic Nerve

-
Slide Long Thoracic Nerve.pdf
-
Download Lecture Overview
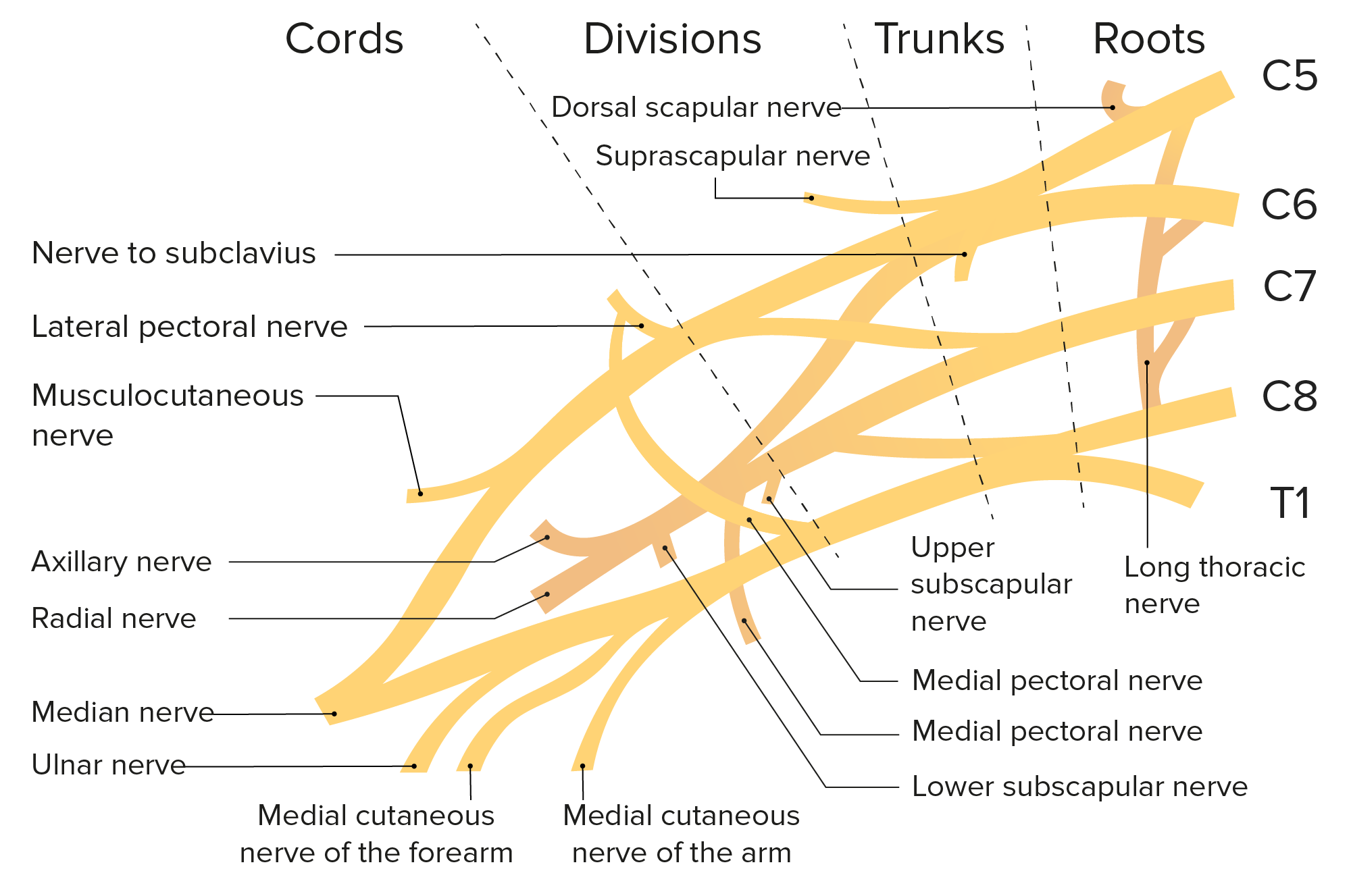
00:01 If we then look at the long thoracic nerve, the course of the long thoracic nerve is really coming high up within the neck. 00:08 So, we can see the anterior rami of C5, C6, C7 forming the brachial plexus. 00:14 And the long thoracic nerve is coming down from this region to run alongside the lateral aspect of the chest wall. 00:20 It's running along the lateral aspect of the chest wall over serratus anterior. 00:25 Here, we're penetrating trauma due to a knife injury if you were stabbed, say, in the chest or something like breast reconstructive surgery can damage this long thoracic nerve as it's running very superficial over serratus anterior which it supplies. If you were to have, like it says, damage to the lateral thoracic wall, then, we would have paralysis of serratus anterior muscle. 00:46 Now, serratus anterior muscle is important in holding the scapular flush against the posterior thoracic wall. 00:54 If the serratus anterior muscle is now paralyzed, the scapula is free to float in the skin of the back and this is what's known as winged scapula. 01:04 The medial border of the scapula no longer held against the posterior wall of the thorax can actually float and protrude into the skin of the back. 01:13 This is especially seen when the patient is asked to push their arm against a fixed wall and that'll actually prevent any stability of that, of the glenohumeral joint and the scapula will push out into the skin of the patient's back. 01:30 So, a number of nerve lesions there which as long as you can remember what the nerve supplies, both its muscle and its sensory distribution, then, locating where that lesion occurs and then, what happens distal to that lesion in terms of muscle supplied and area of the skin covered, that will indicate what the sensory and the paralysis is likely to be.
About the Lecture
The lecture Long Thoracic Nerve by James Pickering, PhD is from the course Fasciae and Neurovasculature of the Upper Limbs.
Included Quiz Questions
Which muscle is paralyzed when the long thoracic nerve is injured?
- Serratus anterior
- Pectoralis major
- Pectoralis minor
- Deltoid
- Trapezius
Author of lecture Long Thoracic Nerve

James Pickering, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
