Playlist
Show Playlist
Hide Playlist
Intraparenchymal Hemorrhage

-
Slides Head Trauma Intraparenchymal Hemorrhage.pdf
-
Download Lecture Overview
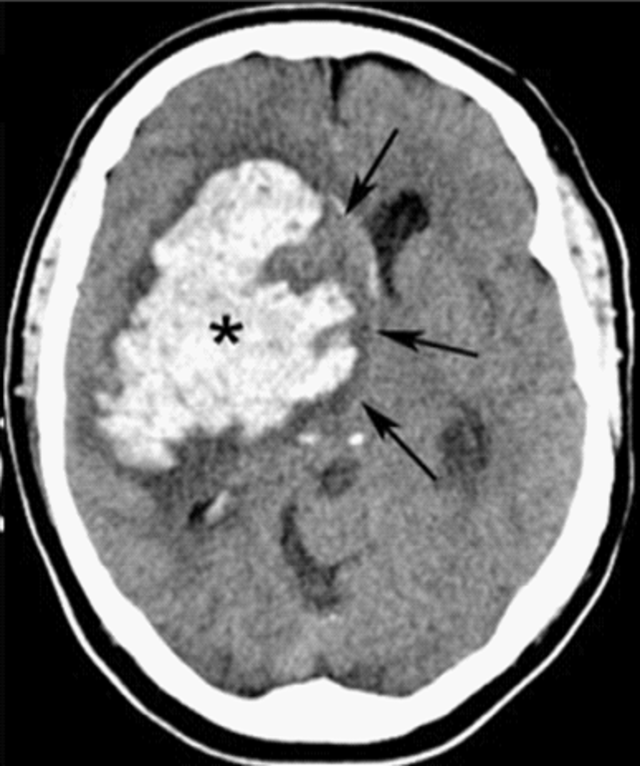
00:01 So let's talk a little bit more about intraparenchymal hemorrhage and start with the definition. 00:06 Intraparenchymal hemorrhages refer to a spontaneous or traumatic bleed into the brain parenchyma. 00:12 This is the second most common cause of hemorrhagic cerebrovascular accidents and also common complication of traumatic brain injury. 00:21 When we think about hemorrhagic strokes, there's subarachnoid hemorrhage, and intraparenchymal hemorrhage. 00:26 So this is a type of hemorrhagic stroke. 00:30 When we think about what's happening in the brain, this schematic again can be helpful. 00:34 We're starting at the surface of the brain outside the brain in the skull and moving down to the parenchyma. 00:39 And here we're looking at hemorrhages that occur in the brain itself. 00:42 These patients present with focal neurologic deficits, small hemorrhages that may not be associated with mass effect and midline shift and increased ICP, and larger hemorrhages may be associated with mass effect, midline shift and increased ICP. 00:57 The location of that hemorrhage in the brain is going to determine the types of symptoms that patients present with. 01:04 In terms of etiologies, there are a number of different causes of intraparenchymal hemorrhages. 01:09 Hypertensive hemorrhages occur in the deep subcortical structures. 01:13 Vascular malformations like AVMs or cavernous angiomas or dural AV fistulas. 01:19 Brain tumors both primary and metastatic brain tumors. 01:23 Cerebral amyloid angiopathy, hemorrhagic transformation of an acute stroke often at that 3-5 or up to 7-day period after an ischemic stroke when the vessels are friable. 01:33 Trauma and other causes. 01:36 Sometimes infection and CNS structures can do it particularly if there's a shower of infectious endocarditis, infectious emboli, there can be an increased risk of hemorrhage in the setting of an infection. 01:49 In terms of diagnosis, again, non-contrast head CT is how we diagnose these hemorrhages. 01:55 It should be performed emergently, we're looking for the location of the hemorrhage. 01:59 We're stratifying surrounding edema and looking at other underlying factors that could point us into a specific etiology. 02:08 To distinguish between ischemic stroke and intracranial hemorrhage, non-contrast head CT should be performed emergently in patients presenting with an acute rapid onset of a focal neurologic deficit. 02:21 In patients where there's ICH or intracranial hemorrhage, we manage the hemorrhage. 02:25 In patients where there's not ICH, patient should be evaluated for IV tPA thrombectomy or for acute interventions for a stroke. 02:34 Follow up imaging is important. 02:35 We need to stratify whether the hematoma hemorrhage is expanding or not. 02:39 And so typically repeat CT or MRI are appropriate. 02:43 We evaluate for neurologic deterioration in the interval and patients with neurologic deterioration should undergo stat imaging or rapid imaging in between surveillance scans. 02:53 Confirmation that hematoma stabilization is important and typically, we will perform follow up imaging at 12 or 24 hours after the initial image. 03:02 And brain MRI with contrast is a modality of choice to evaluate for underlying tumor, CTA or MRA can be used to evaluate for vascular abnormalities and MRI can be used also to evaluate for underlying cerebral amyloid angiopathy to figure out what the cause is for the hemorrhage. 03:19 In the setting of trauma MRI may not be needed, as the result as the clinical presentation of a traumatic event followed by an intraparenchymal hemorrhage may satisfy a definitive diagnosis. 03:31 In terms of management, timely assessment in the ICU or in the hospital is necessary for patients with intraparenchymal hemorrhages. 03:40 The goal is to monitor intracranial pressure, follow their neurologic exam monitor for hematoma expansion correct electrolyte abnormalities and coagulopathies. 03:50 Seizures can occur from intraparenchymal hemorrhages particularly those that are out in the lobes or lobar hemorrhages near the cortical surface and should be managed and evaluated. 04:00 Surgical management could include evacuation of the hematoma or decompressive craniectomy. 04:05 But we really defer surgical management only for those patients who have significant neurologic deterioration. 04:11 The hemorrhage and an intraparenchymal hemorrhage is in between normal neural structures. 04:15 Ultimately, that hematoma will resolve and go down over time and the underlying brain may largely be spared. 04:23 Neurons that have been significantly compressed or damaged as a result of the blood may result in long term neurologic deficits. 04:30 But it's really dramatic the types of improvement and recovery we can see in these patients. 04:34 And so surgical decompression, evacuation or craniectomy are reserved for patients who have significant deterioration despite conservative management.
About the Lecture
The lecture Intraparenchymal Hemorrhage by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What term defines a spontaneous or traumatic bleed into the brain itself?
- Intraparenchymal hemorrhage
- Subarachnoid hemorrhage
- Concussion
- Diffuse axonal injury
- Subdural hematoma
What is a cause of intraparenchymal hemorrhage that occurs in the deep subcortical structures?
- Hypertensive vasculopathy
- Infection
- Amyloid angiopathy
- Glioblastoma
- Arteriovenous malformation
What is the neuroimaging modality of choice to investigate the underlying cause of intracranial hemorrhage?
- MRI with contrast
- MRI without contrast
- CT with contrast
- CT without contrast
- CT angiography
Author of lecture Intraparenchymal Hemorrhage

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
