Playlist
Show Playlist
Hide Playlist
Insomnia: Management

-
Slides Insomnia AcuteCare.pdf
-
Download Lecture Overview
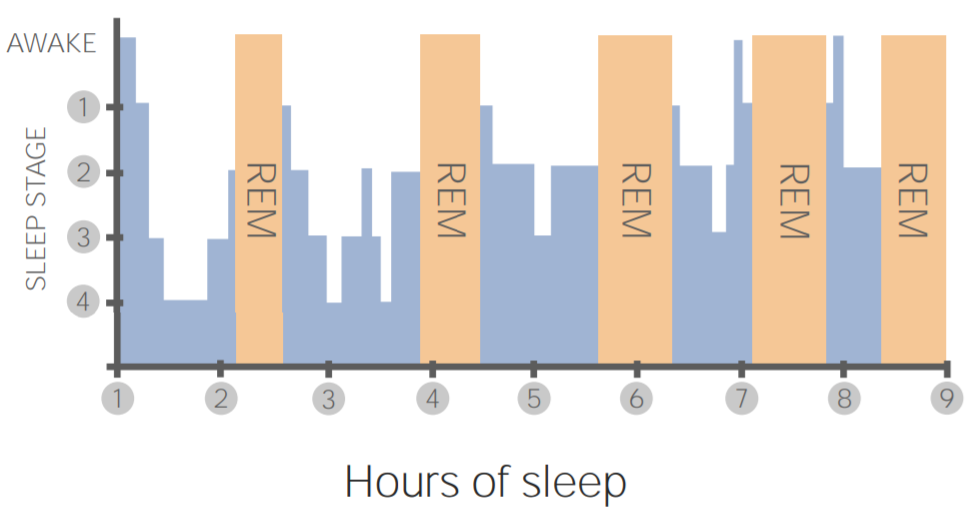
00:01 In terms of treatment of insomnia, I wouldn't rush right to a sleep study or right to doing a bunch of laboratory testing. 00:10 Start with a sleep diary to actually document what's going on. 00:13 Think about those conditions that can make insomnia worse. 00:16 Treat their depression, treat pain before ordering a workup and certainly before recommending other hypnotic therapy for sleep, medications. 00:28 And start with some non-nonpharmacologic interventions. 00:32 These are effective. 00:33 They’re safe and they can prove to be helpful in other aspects of health beyond sleep. 00:39 So, moderate intensity exercise definitely helps regulate your cycle and it helps you sleep, but you want to complete that exercise at least four hours before bedtime. 00:48 Avoiding sleep during the day, if somebody is napping two-and-a-half hours during the afternoon, they're going to experience some awakenings and sleep latency. 00:58 That's normal. 00:59 And it has to be cut out if they ever want to sleep fully through the night. 01:03 Of course, limiting caffeine, tobacco and alcohol use is a good idea and not eating at least four hours before going to bed, avoiding any meal during that time as well. 01:15 Now, let’s talk about advice to give the patient with insomnia and just general sleep hygiene. 01:20 First of all, just go to bed when tired. 01:22 The patients who – again, who get into real trouble with insomnia are the ones who really try to force the sleep upon themselves and sleep just doesn't work like that. 01:33 And I think that promotes an anxiety. 01:35 Whether they had anxiety before or not, it promotes an anxiety in trying to sleep and worrying about this problem, such that it self-perpetuates and you're guaranteed to have more insomnia. 01:45 So, use the bed only when tired. 01:49 Use the bedroom only for sleep and for intimacy. 01:51 That's it. 01:52 Try to settle down before bedtime. 01:55 So, do really boring things. 01:56 I don’t know if chess necessarily boring. 01:58 There’s a pawn there, but maybe it’s reading. 02:01 It’s nothing crazy and active and you’re not running around, doing a million chores. 02:06 You do have a little time to settle down. 02:09 And if you wake up, do more boring things. 02:12 And if you do get up, and I think this is one of the most critical things, don't just lie and push yourself to try to sleep. 02:18 That again doesn't work. 02:19 Get up, get out of bed, do something for 20 minutes, 40 minutes and then return when you feel sleepy. 02:26 That one really does work. 02:28 And usually, between these recommendations and the lifestyle recommendations, you’re going to manage about 80 to 90% of insomnia cases effectively, just with these alone. 02:42 So, pharmacologic treatment, limited to the short term. 02:45 The drugs can disturb sleep architecture. 02:49 They have addictive potential. 02:51 And as well, among older adults, they can promote falls and more cognitive problems. 02:57 So, benzodiazepines, they have a higher risk of abuse. 03:00 I really use them for only very limited periods of time, no more than a week generally speaking for those drugs. 03:09 Over-the-counter treatments like diphenhydramine don't work very well, but they can promote some of that cognitive dysfunction, somnolence and falls. 03:18 And finally, just a quick word on melatonin. 03:21 It probably works particularly for switching time zone, but we’re talking about reducing sleep latency by a few minutes on average. 03:29 So, it's probably not something patients are really going to feel as a benefit. 03:33 But if it helps them relax and makes them feel a little bit better, that's great. 03:38 There is a risk of daytime grogginess afterwards as well with melatonin. 03:42 So, it's not a completely benign agent. 03:46 So, this gives you a nice overview of sleep. 03:50 It helps, I think, you to discuss normal sleep and changes with sleep as you age with your patients and then that's a nice entrée for starting to talk about sleep hygiene and how to how to set the right environment and tone for sleep. 04:06 And as I said, that's going to help you with the majority of your patients. 04:09 Thanks very much.
About the Lecture
The lecture Insomnia: Management by Charles Vega, MD is from the course Acute Care.
Included Quiz Questions
What is the most appropriate first-line treatment for short-term insomnia?
- Sleep hygiene
- Benzodiazepines
- Diphenhydramine
- Melatonin agonists
- Zolpidem
Which of the following is NOT recommended for sleep hygiene?
- Practice forcing sleep
- Exercise regularly
- Avoid daytime naps
- Avoid alcohol near bedtime
- Avoid caffeinated beverages after lunch
Which of the following complications is LEAST associated with hypnotic sleep agents?
- Increased anxiety
- Increased falls
- Disruption of sleep architecture
- Daytime somnolence
- Cognitive impairment
What is the most affective treatment for insomnia in a patient with major depressive disorder?
- Treatment of depression
- Benzodiazepines
- Zolpidem
- Diphenhydramine
- Opioids
Author of lecture Insomnia: Management

Charles Vega, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
