Playlist
Show Playlist
Hide Playlist
Inguinal Hernias

-
Slides Inguinal Hernias.pdf
-
Download Lecture Overview
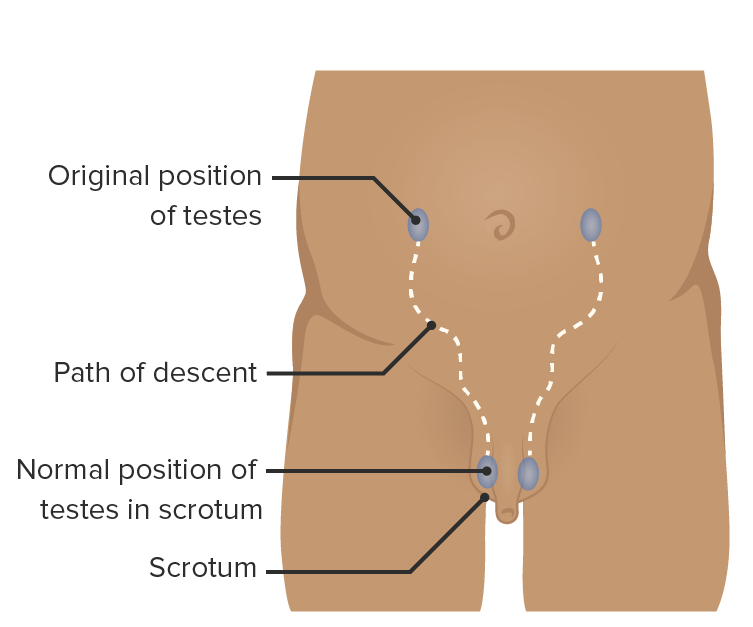
00:01 So now we've covered the anatomy of the inguinal region. 00:04 It's important we look at inguinal hernias. 00:06 A hernia is essentially where a piece of tissue protrudes from its normal location into an abnormal location or region where it doesn't usually occupy. 00:16 As you can imagine, the complex anatomy of this space with various structures normally passing through as part of embryonic and fetal development. 00:24 Now, has left potential weak spots. 00:28 Readers of the anterior abdominal wall where a testes or the round ligament of the uterus of past leave behind these possible weak spots. 00:35 So let's have a look at these as inguinal hernias. 00:38 What we're looking at the moment is quite a complicated diagram. 00:41 So let's try and orientate ourselves. 00:44 What we have is the inguinal ligament passing from the anterior superior iliac spine, which is up on the top right hand corner. 00:51 All the way down to the pubic tubercle, down towards the bottom left. 00:54 That's the inguinal ligament you should be familiar with. 00:58 On the left hand side we can see the vertical muscle of rectus abdominis. 01:01 And on this right hand side, we can also see iliopsoas muscle, which is lining the lateral aspect of the pelvis. 01:08 We can also see running alongside that but underneath a layer of fascia, the femoral nerve. 01:13 And here we can see the femoral artery and vein. 01:16 These are passing through the pelvis under the inguinal ligament to pass into the lower limb. 01:21 And this is part of what's known as the subinguinal space, a space that sits underneath the inguinal ligament. 01:29 We're interested in this region that sits above it. 01:32 Here we have a layer of transversalis fascia that lays on this region. 01:36 And we have the opening of transversalis fascia, which is the deep inguinal ring. 01:42 So here we can see transversalis fascia. 01:45 And now if you imagine a testee passing through the transversalis fascia at the level of the deep inguinal ring, we can see we now have this opening. 01:55 What we can see that's lying medial to the deep inguinal ring are the inferior epigastric vessels. 02:03 So here we can see we have the deep inguinal ring lying medial to the deep inguinal ring. 02:08 We have the inferior epigastric vessels. 02:11 And they're running in and supplying things like rectus abdominis. 02:15 What we can then see is between the inferior epigastric blood vessels and rectus abdominis we have this small little inguinal triangle known as inguinal or Hesselbach triangle. 02:28 So the medial border there is the lateral edge of rectus abdominis. 02:33 The lateral border is the inferior epigastric vessels, and the inferior border is the inguinal ligament. 02:40 The inguinal triangle is between those three boundaries, and that's where you would find the superficial inguinal ring. 02:48 Now we can remember that the superficial inguinal ring is the exit point of the testes or the round ligament of the uterus. 02:54 And it's a defect and opening within the aponeurosis of external oblique. 02:59 It's reinforced posteriorly by the conjoint tendon. 03:03 We can see in this diagram where you can see the male penis you can see just to the right and above the penis a bulge which is not present on the left hand side of the screen. 03:13 That is because a piece of tissue perhaps a piece of small intestine has taken advantage of this space. 03:19 This weakness and protruded through the superficial inguinal ring and you can see it manifesting itself as this bulge just above the external genitalia where the mons pubis is located. 03:33 If we want to have a look at an indirect inguinal hernia, and what I was referring to previously is what's known as a direct inguinal hernia. 03:40 But an indirect inguinal hernia is one where a piece of tissue would move very much towards that same location. 03:47 So again, moving into this direction but it would take much more of an indirect pathway. 03:53 So clearly you can see why a direct inguinal hernia is passing to that same location, but it's taking a direct pathway to it by going through the superficial inguinal ring. 04:05 It's passing directly to that region. 04:08 If we were to think more of an indirect route, how could you get to that region? You'd pass through the deep inguinal ring. 04:16 So this time, you'd pass through the deeping ring, and then actually pass through the same structures that the spermatic cord passed through as you went in that direction. 04:28 So this time, you've got this potential space, which is where the spermatic cord are running. 04:33 And you can see how a piece of small intestine covered by parietal peritoneum could now exploit this space, but this time, potentially pass all the way into the scrotal sac. 04:46 So it could initially look like it's just a mound above the external genitalia. 04:51 But with continued intra-abdominal pressure, it could pass all the way through into the scrotal sac because it's following the same path as the testes did going through forming the spermatic cord. 05:04 And the contents of that would also be covered by the spermatic cord. 05:09 This just looks at the direct inguinal hernia again, instead of being the indirect route, we're now looking at the more direct route, which is exploiting the superficial inguinal ring within the inguinal triangle. 05:20 So it's taking that path very much going directly through the superficial inguinal ring, but it's not going through the deep inguinal ring. 05:29 The major landmarks used to determine a deep direct from an indirect is on an ultrasound to find the inferior epigastric blood vessels and where you have a bulge medial to the inferior epigastric vessels. It will be a direct. 05:47 And where you have it lateral to the inferior epigastric blood vessels, it will be indirect. 05:51 And here we can see the risk of passing through medial to the inferior epigastric blood vessels. 05:58 It won't make its way into the scrotum, but it will still form a bulge just above the external genitalia.
About the Lecture
The lecture Inguinal Hernias by James Pickering, PhD is from the course Anterolateral Abdominal Wall.
Included Quiz Questions
At which position related to the inferior epigastric vessels do indirect inguinal hernias occur?
- Lateral
- Medial
- Inferior
- Superior
- Anterior
Which statements regarding indirect inguinal hernias are accurate? Select all that apply.
- They are congenital.
- The contents usually go into the upper thigh.
- They occur lateral to inferior epigastric vessels.
- They are caused by failure of embryonic closure of the processus vaginalis.
- They are less common than direct hernias.
Which nerve passes through the superficial inguinal ring and can be injured during hernia repair?
- Ilioinguinal nerve
- Pudendal nerve
- Iliohypogastric nerve
- Subcostal nerve
- Obturator nerve
A patient presents with pain in his scrotum. Examination findings show that he has an indirect inguinal hernia that is compressing a nerve. Which nerve is responsible for the patient's pain?
- Ilioinguinal
- Iliohypogastric
- Genitofemoral
- Subcostal
- Obturator
Which structures pass through the deep inguinal ring in women?
- Round ligament of the uterus
- Ilioinguinal nerve
- Iliohypogastric nerve
- Spermatic cord
- Broad ligament of the uterus
What is known about a direct inguinal hernia?
- It occurs at the level of the superficial inguinal ring.
- It occurs at the level of the deep inguinal ring.
- It exits the abdomen lateral to the inferior epigastric vessels.
- It is typically found in young men.
Author of lecture Inguinal Hernias

James Pickering, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
