Playlist
Show Playlist
Hide Playlist
Hypothyroid and Hyperthyroid Myopathy

-
Slides Toxic Myopathies.pdf
-
Download Lecture Overview
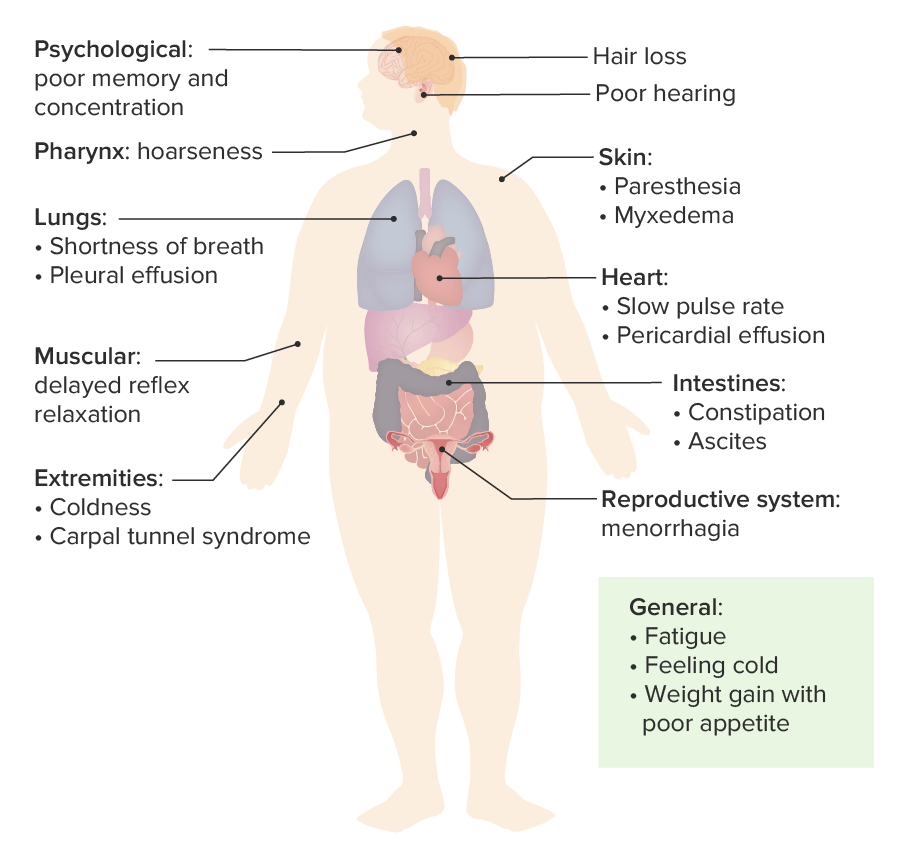
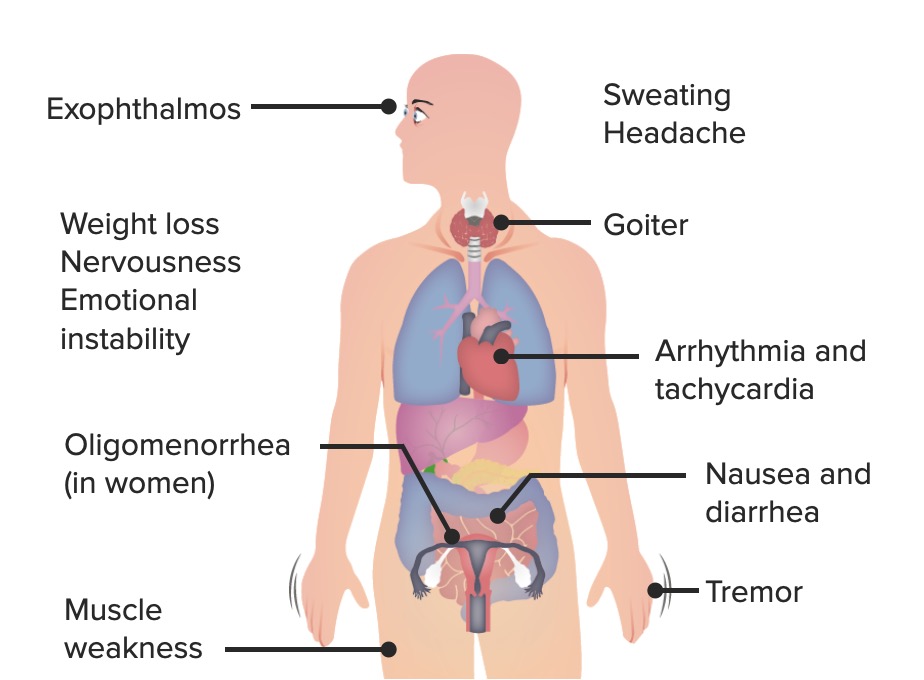
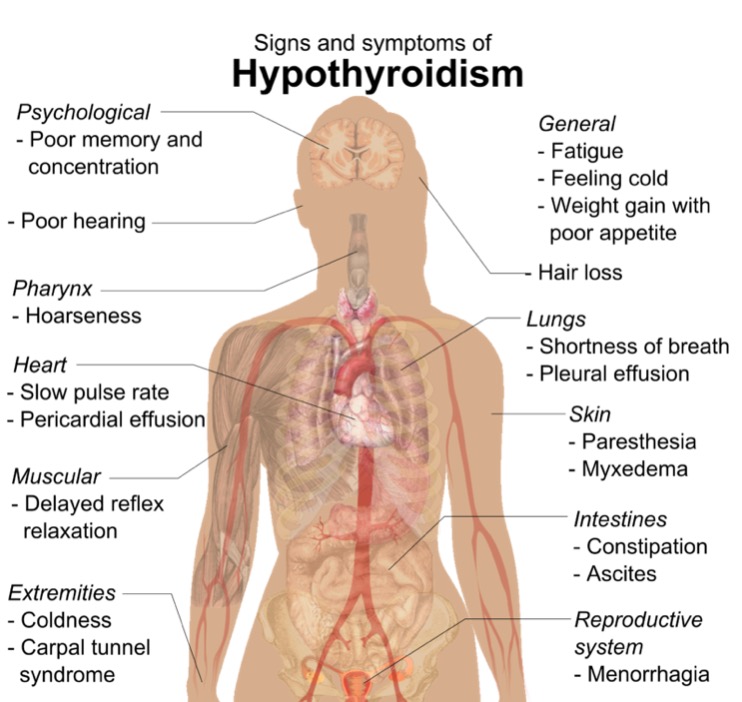
00:00 So let’s start with hypo and hyperthyroid myopathy. Both too low thyroid function and too high thyroid function can affect the muscle. The thyroid is that gland in the neck that’s a critical regulator of energy within the cells. And then too much or too little can cause problem with the muscle, a highly metabolically active organ. Let’s start with hypothyroid myopathy. This presents with subacute to chronic onset of symptoms and typically we see muscle weakness that looks like a myopathy. Patients have proximal weakness more than distal. We can see myalgias and muscle cramps, and we even see this interesting finding of myoedema. This is where a percussion hammer, which is struck against the muscle, will cause a small lump to develop in the muscle when it is struck. Importantly, when we see hypothyroid myopathy or T4 deficiency, this leads to myopathy through a number of metabolic changes; abnormal glycogenolysis, mitochondrial oxidative metabolism, triglyceride turnover, all of those can contribute to impaired muscle function and cause this type of myopathy. Similarly, we can see myopathic presentations in patients who are hyperthyroid. Again, this is typically subacute more so than chronic. The presentation is similar to hypothyroid myopathy with proximal weakness. Myalgias are less common. We don’t see cramps. And we also don’t see this myoedema phenomenon. So it’s important when evaluating a patient who has a myopathic presentation; proximal weakness, normal sensation, normal reflexes, to look for thyroid dysfunction or test thyroid studies. So what is the workup? Well, for hypothyroid myopathy, we see increased TSH, because the pituitary is telling the thyroid to work and it’s not working. 01:57 We see reduced T4. Literally, there is less thyroid hormone leaving the thyroid. And we can see slightly increased CK levels. And that’s very uncommon for a toxic myopathy. Typically, we think of CK as indicating inflammation in the muscle and when the CK is elevated, we look at inflammatory myopathies. When the CK is normal, we think about toxic myopathies. And hypothyroid myopathy is one exception where slightly elevated CKs in the hundreds can be present in those patients. What’s the management? To correct the thyroid dysfunction and we see that CK levels quickly fall with treatment. TSH levels normalize later and weakness recovers most slowly. What about with hyperthyroid myopathy? Well here, we see the CK is normal, follows the typical pattern for a toxic myopathy. An EMG nerve conduction study, the EMG can show myopathic motor units. Short duration, small amplitude, small muscle units and fibrillation potential activity is usually absent. There’s not evidence of active inflammation with the fibrillation potentials. And pathologic changes are typically nonspecific, the biopsy doesn’t help. The goal for management is to return patients to euthyroidism and patients generally improve over the course of months.
About the Lecture
The lecture Hypothyroid and Hyperthyroid Myopathy by Roy Strowd, MD is from the course Acquired Neuromuscular Diseases.
Included Quiz Questions
Which of the following is characteristic of hypothyroid myopathy?
- Myoedema
- Brisk ankle reflex
- Difficulty in swallowing
- Peripheral neuropathy
- Bilateral hand tremor
Which of the following laboratory findings is consistent with hyperthyroid myopathy?
- Normal creatine kinase
- Elevated thyroid-stimulating hormone (TSH)
- Low thyroxine (T4)
- High erythrocyte sedimentation rate (ESR)
- Low serum creatinine
Author of lecture Hypothyroid and Hyperthyroid Myopathy

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
