Playlist
Show Playlist
Hide Playlist
Hypertensive Retinopathy

-
Slides OP Retinopathies.pdf
-
Download Lecture Overview
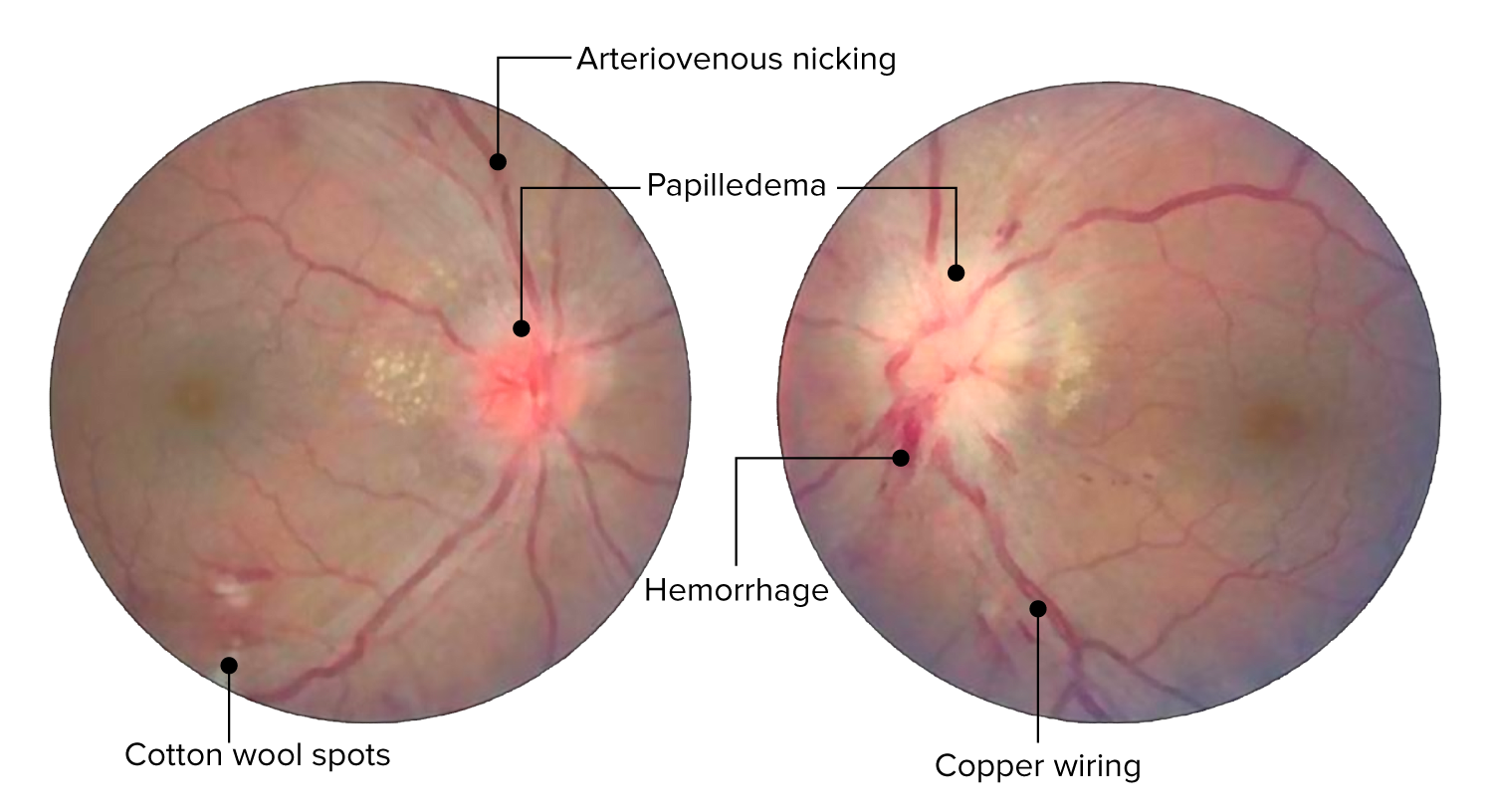
00:00 Finally, Hypertensive Retinopathy. Relatively common because hypertension is a big deal or very common pathology we see in the human condition. It's going to be due to elevated systemic and then specifically elevated retinal artery pressures. So what's going on here? There are different faces in the pathophysiology in the development of hypertensive retinopathy. So, in the vasoconstrictive phase, so the eye wants to very carefully regulate the blood pressure into the eye so if there is increased systemic pressure coming in through the retinal artery, the artery responds by doing reflex of vasoconstriction that reduces the flow and so you'll get generalized retinal artery narrowing. That keeps the pressure appropriate into the eye, but that reflex vasoconstriction is also going to be a nidus, an area where we will have a preferential development of atherosclerotic vessel segments. Now, those vessels, with that kind of change, cannot have improved vascular flow when they need it and so there is a relative now obstruction to flow that is reducing flow into the eye, but also causing much higher flow retrograde. And that higher pressure retrograde is going to be reflected in a number of manifestations. So, we are going to get ruptured vessels. These are relatively thin-walled arterioles so we will get in the eye that we can see on fundoscopic exam a flame-shaped hemorrhage, so-called flame shaped. Literally it kind of a rupture of the blood vessel and so-called dot blot hemorrhages. Again, rupture, focal, discontinuities within the arterioles. We will get microaneurysms as we get vascular outpouching as a result of the increased retrograde pressure. We will get accumulation of lipid and protein because under increased pressure we will get exudates that accumulate. So we will see hard exudates that are associated with this. And now because of this area in the middle where we have increased atherosclerotic damage, then we're going to get retinal ischemia and microinfarcts and so we'll see cotton wool spots. That's what's going on with hypertensive retinopathy. 02:37 Here's a pretty gnarly looking 2 eyes associated. So the fundoscopic exam in a patient who has such severe end-stage hypertensive retinopathy, the cotton wool spots that we're seeing there identified or retinal ischemia microinfarcts. There will be hemorrhages again because we have ruptured the blood vessels with all that proximal increase in blood pressure. We'll have papilloedema. So this is due to ischemia of the optic nerve with swelling and you see an increased pallor around the optic disc. There will be arteriovenous nicking. 03:15 So, when you look very carefully there, you see that that vein as it's going along suddenly seems to have a discontinuity in that. Well that's because that there is a thickened arteriole that's crossing that, compressing it, and narrowing that venule that gives you the apparent nicking on the fundoscopic exam. And you'll see copper wiring. So normally an arteriole has a kind of a central clear yellow area. This gets accentuated. The light reflex that allows us to see artery versus vein on a fundoscopic exam is accentuated in the setting because of their arteriosclerotic changes that are happening in the vessel with chronic hypertension. Now most patients even with systemic hypertension, most hypertensive patients are asymptomatic and that's true of the hypertensive retinopathy. They may not be aware at all that there is anything going on until much further along distally in the disease near the end. They may get headaches with papilloedema, that pressure on the optic nerve, you will get headaches and can get nausea and vomiting as well in severe cases. Because of the papilloedema, because of the excess water in the interstitial connective tissue, we're going to see decreased or blurry vision and you can get vision loss but this usually occurs as a secondary consequence of optic atrophy and/or retinal detachment. And with that, we have covered kind of 3 major retinal diseases; diabetic retinopathy, retinopathy of prematurity, and hypertensive retinopathy. Hope you enjoyed it.
About the Lecture
The lecture Hypertensive Retinopathy by Richard Mitchell, MD, PhD is from the course Posterior Segment Eye Diseases.
Included Quiz Questions
What is characteristic of the exudative phase of hypertensive retinopathy?
- Flame-shaped/dot-blot hemorrhages
- Pinpoint/petechial hemorrhages
- Pinpoint/purpuric hemorrhages
- Flame-shaped/petechial hemorrhages
- Flame-shaped/blot-shaped hemorrhages
What causes most of the signs and symptoms of hypertensive retinopathy?
- Papilledema
- Retinitis
- Retinal detachment
- Macular degeneration
- Optic nerve palsy
Author of lecture Hypertensive Retinopathy

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
