Playlist
Show Playlist
Hide Playlist
Human Immunodeficiency Virus (HIV): Diagnosis and Management


-
Slides HumanImmunodeficiencyVirus InfectiousDiseases.pdf
-
Download Lecture Overview
00:01 So we’ve got to temper this if we have such a reaction in a patient. 00:07 Even though they’re still getting the antiretroviral therapy, we’ve got to temper this if we possibly can by giving them NSAIDs, non-steroidal anti-inflammatory drugs, if they have just mild symptoms. 00:21 But we may have to go ahead and give them corticosteroids as much as we’d like to avoid suppressing their immune system. 00:28 But then again, the manifestations of, for example, their cryptococcal meningitis may be worse once their immune system is coming back. 00:38 And then we have to deal with the risk of the corticosteroids with hyperglycemia, increasing blood pressure, confusion, worsening of the existing infection, and then predisposition to a new infection. 00:52 So it’s kind of a very tightrope that we’re walking in this immune reconstitution inflammatory syndrome, also known as IRIS. 01:04 So let’s say you have documented IRIS. 01:10 When do you initiate antiretroviral therapy in a patient with a recent opportunistic infection? Let’s say you diagnosed the opportunistic infection first. 01:21 Should you start them on therapy? Well, it’s better to go ahead and treat their opportunistic infection first and make sure that they are tolerating that therapy. 01:34 And then you can switch them to either a more active and/or begin the first initiation of antiretroviral therapy. 01:46 So what are some examples? We talked about viruses, fungi, and bacteria, including the mycobacterial, and some patient examples that I want to point out that I’ve seen would be activation of CMV retinitis – a sight-threatening lesion. 02:03 There’s not much room in the eye for an inflammatory reaction, so we don’t want IRIS in the eye. 02:11 And then I mentioned in passing activation of symptoms of cryptococcal meningitis. 02:19 This usually begins 4-8 weeks after either beginning or changing therapy. 02:26 What’s happening once again is the immune system is coming back. 02:30 What about testing patients for HIV infection? The counseling that you do is extraordinarily important. 02:42 One of the first points of counseling would be to tell the patient why you think an HIV test is necessary, and that requires just right doctoring. 02:56 It requires concern and compassion. 02:59 And you need to preface it by saying that, “Should you prove to have HIV infection, we’ve got great treatment for it nowadays." So it’s not any longer a death sentence. 03:13 In the early ’80s, it was a death sentence when we couldn’t do much about it. 03:17 But we’ve got treatment now that can allow patients to live out a fairly normal lifestyle. 03:25 We need to talk to them about their risks – what is their risk of acquiring infections. 03:33 For example, if they live in the desert Southwest or if they live in the Ohio, Mississippi River Valley, or other endemic areas where certain fungal infections are likely, they need to report new symptoms to their physician. 03:50 We need to discuss the limitations of the various assays that we do to measure their CD4 T-cell count. 03:58 We need to talk to them about the implications of positive test results, and we need to reassure them of our confidentiality, their concern, and that we want to follow them up. 04:13 With physicians like this, we had the best chances for a good outcome. 04:20 So we do this laboratory testing and now there are 4th generation immunoassays for HIV-1 and -2, so we can easily detect this infection. 04:32 Now if you’re trying to discern whether the patient has an acute retroviral syndrome, the acute HIV infection, we use something called the P24 assay. 04:45 This P24 antigen is a particle on the surface of the HIV. 04:53 If the results of HIV testing are completely negative, there’s nothing else to do – no further testing except perhaps to counsel the patient about the ways that HIV is transmitted and announce to them if they're in a risk group, that they should be very, very careful. 05:13 If the results are positive, we don't automatically assume they're positive. 05:20 We repeat the 4th generation immunoassay. 05:24 If the results come back indeterminate, then we’re going to do something called measuring an HIV viral load, which is the way we measure the presence of HIV-1 nucleic acid in the bloodstream. 05:41 So the evaluation before beginning treatment is going to include a CD4 count, an HIV viral load, and we’re going to test viruses for resistance to antiretroviral therapy because the resistance is not inconsequential. 06:00 It’s probably at least 4 to 10 percent of HIV are resistant to various classes of antiretroviral therapy. 06:10 We’re going to check them for hepatitis B and C. 06:14 We’re going to get some basic chemistries. 06:17 We’re going to test their liver enzymes because some of the treatment we may use could adversely affect their liver function. 06:25 We’re going to get a CBC with a differential white count. 06:29 And because some of these antiretroviral agents affect lipids, we’re going to get a fasting lipid profile. 06:37 We’re going to get a fasting glucose and hemoglobin A1C because not only are some patients diabetics, but some of the antiretroviral therapy can aggravate glucose tolerance. 06:51 We’re going to get a urinalysis because one of the things that can happen is HIV nephropathy. 06:58 And certainly in women, we’re going to get a pregnancy test so that we know how to protect the baby. 07:04 So how do we treat HIV infection? In the early to mid-1980s, a drug called AZT was introduced – azidothymidine. 07:16 We thought that this was going to work very well. 07:20 And it indeed decreased the viral load and increased the CD4 count. 07:27 But unfortunately, it lasted only a few months, and then the virus apparently developed resistance to it. 07:36 We tried the same experiment with two drugs. 07:40 Two, we thought, might be better than one, but the same outcome. 07:44 The virus could get used to two drugs. 07:47 So it turns out that the virus has trouble if you throw three drugs at it, that’s why we start all the patients essentially on triple drug therapy. 07:59 So HIV becomes resistant to one or two. 08:05 And so, we have now several classes of antiretroviral agents. 08:12 We have agents that block the fusion of the virus with the cell. 08:18 We have reverse transcriptase inhibitors. 08:21 We’ve got protease inhibitors. 08:23 We’ve got integration inhibitors. 08:25 And so, we’ve got a whole group of agents that we can choose. 08:30 If the virus might be resistant to one class, we can choose others. 08:34 There’s a lot of weapons we have to throw at this particular virus. 08:39 And what I’ve listed for you here are essentially all the classes of antiretroviral agents. 08:48 And I believe this is beyond the scope for step 1, 2, or 3 testing because most patients are referred to infectious disease specialists. 09:03 We need to know the details of the toxicity and the indications for these, but I think it’s premature to suggest that you need to know all of these details. 09:14 In case you might be interested in further reading about it, we have downloaded all of these agents and their toxicity to this package that we’re presenting. 09:27 What we should talk about is the toxicity that’s common to all antiretroviral agents, and number 1 is gastrointestinal upset. 09:38 Number 2 is lipodystrophy. 09:42 And so, lipodystrophy can include lipoatrophy with fat loss, and this includes the buckle fat pads, the extremities, and the buttocks. 09:57 And I need to tell you an interesting patient that I had who was doing beautifully on the 3-drug therapy that I had prescribed for him. 10:05 But he came in to me on a follow-up visit and said, “Doc, you’ve got to change my regimen. 10:13 This regimen that you gave me has outed me and people know I’m HIV-positive. 10:21 I haven’t told them, but they know I’m HIV-positive because of the changes in my face. 10:28 I’ve lost some of the tissue in my face.” What he was referring to is he’s lost some fat in the buckle fat pads. 10:37 And I couldn’t tell the difference, but he could tell the difference. 10:42 And apparently, his friends had noticed a change in his face. 10:46 So I did switch regimens because he wanted to be confidential about his HIV status. 10:56 I thought that’s an interesting patient that I saw. 11:00 Once I changed the regimen, on follow-up visits he came back to me very happy. 11:06 The other thing that can happen is, not only atrophy, but excessive central fat deposition. 11:14 Previously, very athletic-looking young men with flat abdomens were developing papa bellies – a swollen abdomen – or they were getting a buffalo hump at the nape of their neck, or in the suprapubic area. 11:33 In men, breasts were enlarging. 11:35 And so, these are toxicities that are common to all of the agents. 11:41 Now, which agent specifically does one more than the other, whether it’s protease inhibitors, non-nucleoside reverse transcriptase inhibitors, or the combination, I don’t think the data are very clear about that.
About the Lecture
The lecture Human Immunodeficiency Virus (HIV): Diagnosis and Management by John Fisher, MD is from the course Genital and Sexually Transmitted Infections. It contains the following chapters:
- IRIS – Management
- HIV – Diagnosis
- Laboratory Testing
- HIV Infection – Management
Included Quiz Questions
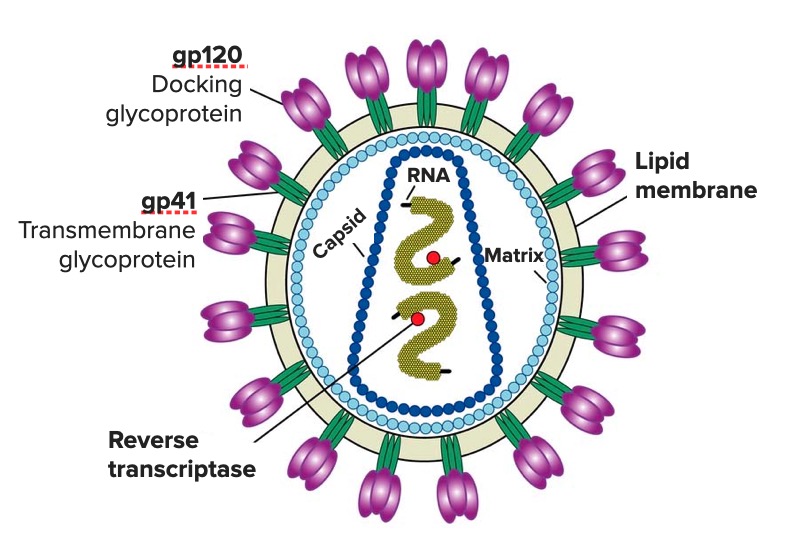
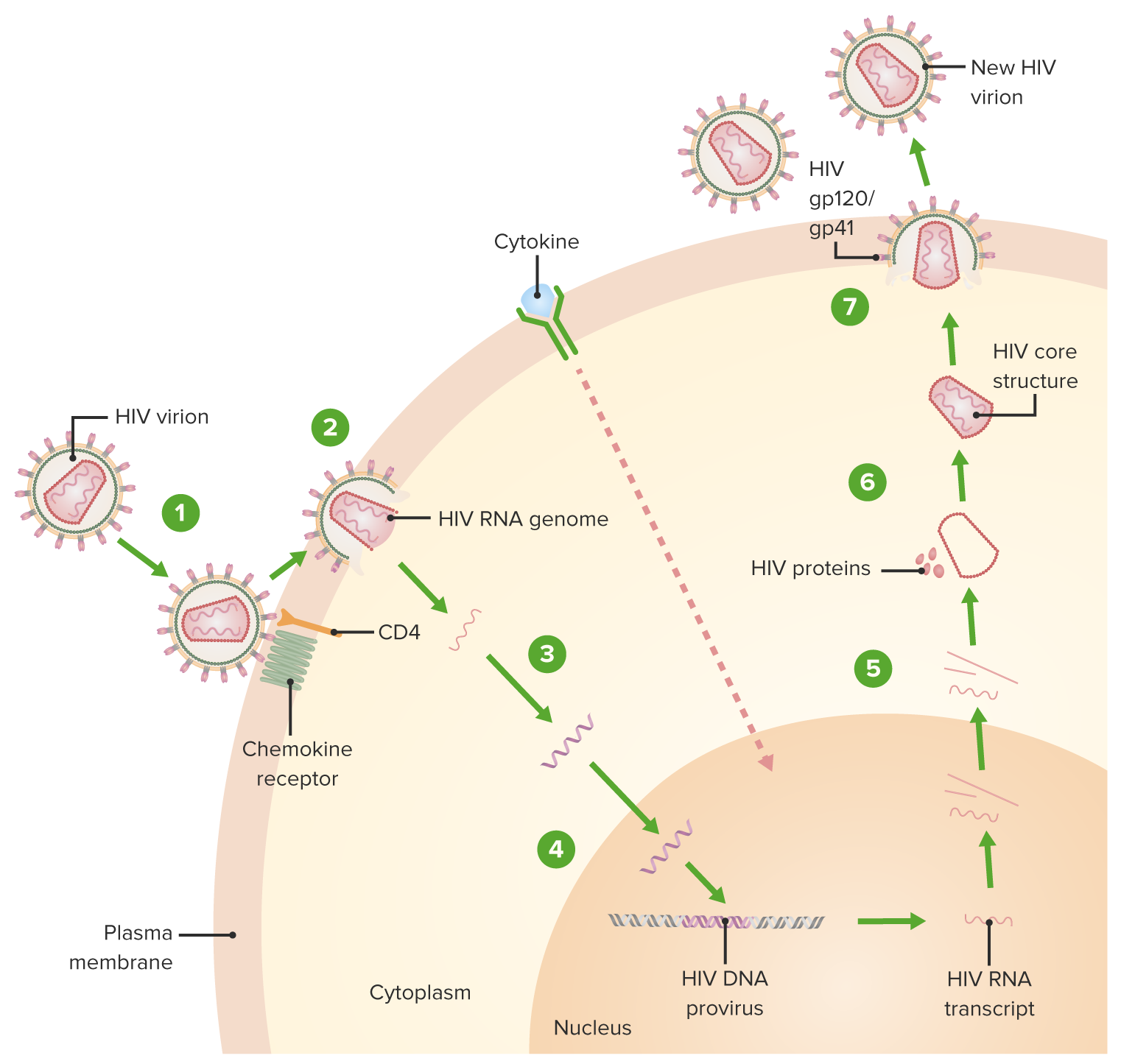
Fusion inhibitors prevent viral fusion to CD4 cells by binding to which of the following envelope receptors?
- Glycoprotein 41
- C-C chemokine receptor type 5 (CCR5)
- Glycoprotein 120
- C-X-C chemokine receptor type 4 (CXCR-4)
What is the mechanism of action of reverse transcriptase inhibitors?
- Competitive binding to viral reverse transcriptase
- Competitive binding to host cell reverse transcriptase
- Competitive binding to host cell helicase
- Competitive binding to retroviral helicase
- Competitive binding to viral and host cell reverse transcriptase
What is the best step after a positive fourth-generation HIV-1/2 immunoassay?
- Further serology testing
- Initiation of antiviral therapy
- Viral RNA
- Viral cultures
A fasting blood glucose and lipid panel is performed in patients diagnosed with HIV infection. This is primarily due to which of the following reasons?
- Hyperlipidemia and hyperglycemia can be worsened by some anti-retroviral therapies.
- HIV causes metabolic syndrome in most patients.
- Patients with metabolic disorders often have more severe HIV infection.
- Ketoacidosis and pancreatitis are more common in such patients.
Which of the following statements regarding antiretroviral medications and lipodystrophy is MOST ACCURATE?
- It is a common side effect of most antiretroviral medications.
- It occurs more commonly with newer antiretroviral medications.
- It is not a side effect of antiretroviral medications.
- It is a rare side effect of most antiretroviral medications.
Which of the following is the most appropriate antiviral therapy for treatment-naïve HIV-infected patients?
- Triple drug therapy
- Low-dose single drug therapy
- High-dose single drug therapy
- Low-dose double drug therapy
- High-dose double drug therapy
Author of lecture Human Immunodeficiency Virus (HIV): Diagnosis and Management

John Fisher, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Focuses on the highlights and omits the extraneous details. Felt as though this has helped me master HIV a bit better
I'd would have like to know where western blots fit in the diagnostic pathway. I think in Australia after positive confirmation of p24 go on to perform westernblots. Also what about the impact the window period has and the new for follow up testing? Finally it would have been good to discuss what is considered to be as treatment failure with HAART.
