Playlist
Show Playlist
Hide Playlist
Introduction & Graves' Disease – Hyperthyroidism (Thyrotoxicosis)


-
Slides Hyperthyroidism incl. Graves Disease.pdf
-
Download Lecture Overview
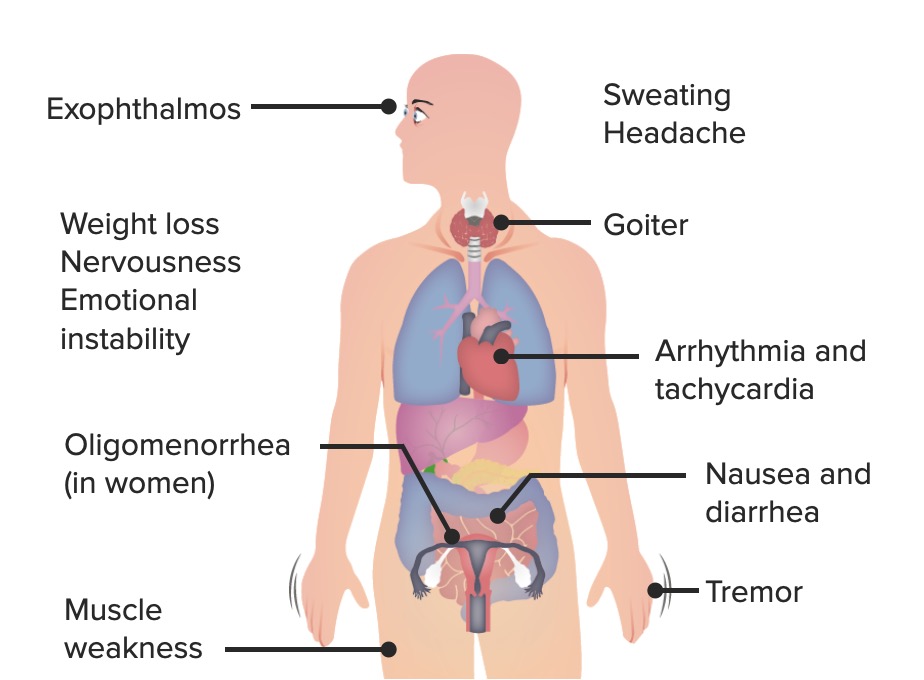
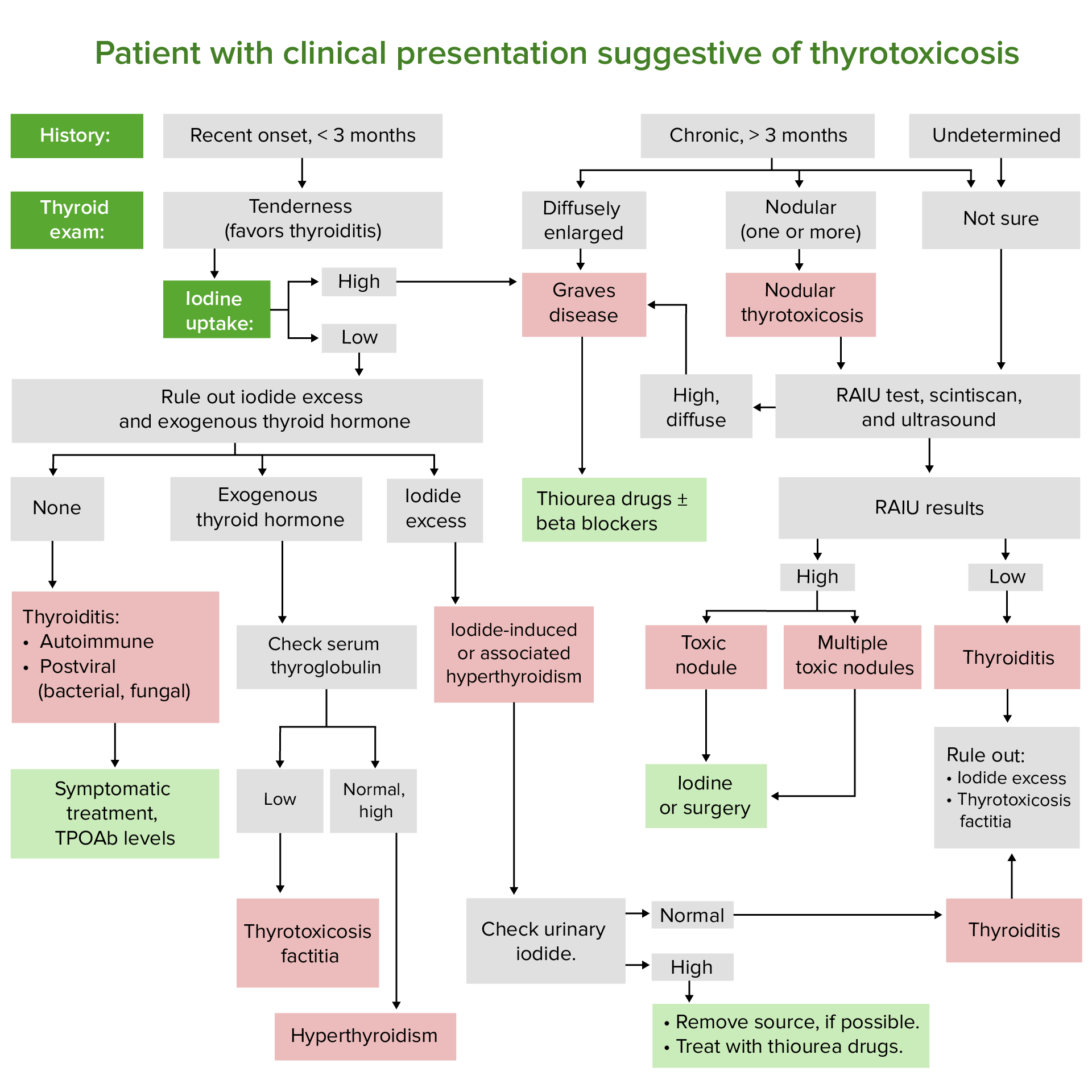
00:01 Hypothyroidism is where we are. 00:03 Think about your patient walking through the door. 00:06 Anxious, palpitations, sweating, eating quite a bit of food, but yet is not gaining weight. 00:14 What we’ll take a look at with hyperthyroidism and then differentials for you; in other words, thyrotoxicosis. 00:19 Something’s causing your thyroid gland to increase production of T3, T4. 00:23 Maybe Graves’, thyroiditis, iodine-induced, choriocarcinoma… why? Human chorionic gonadotropin replaces TSH. 00:31 Pituitary tumour, what are you releasing? TSH. 00:37 Struma ovarii, where are you? Ovaries. 00:42 How is that causing hyperthyroidism? Struma ovarii, it’s part of a female teratoma in the ovaries producing directly T3, T4. 00:53 Topic, hyperthyroidism… patient has too much T3, T4 for whatever reason… look at the differentials. 01:01 Exogenous… absolutely or perhaps even you have a patient that has hypothyroidism taking synthroid excessively resulting in hyperthyroidic type of symptoms. 01:16 We’ll begin our discussion by looking at Graves’. 01:19 Let me set this up for you. 01:21 On your left, you see that grey blob? Hahaha, well, that grey blob; in other words, that’s your thyroid gland and on your basolateral membrane, you have a TSH receptor. 01:33 Do you remember that? And that TSH receptor regulates whom? That’s important known as your sodium-iodide symport. 01:40 As long as everything’s perfectly normal, you have a proper feedback mechanism in place. 01:44 The TSH will bind to the receptor and you will have increased production of one lightning bolt. 01:51 What does that lightning bolt represent? T3,T4. 01:56 Just right so you can maintain normal basal metabolic rate… BMR versus Graves’, what’s happening? Oh, the TSH is being replaced by whom? An immunoglobulin antibody known as TSI, thyroid stimulating immunoglobulin. 02:14 When you have an immunoglobulin that is then attacking in this case, remember when I say attack, it could either destroy it like myasthenia gravis or it could stimulate it, as you would have here. 02:23 So, it’s a type II hypersensitivity. 02:24 It is bind to your TSH receptor and what’s it doing? Take a look at the number of lightning bolts… cute perhaps; if not, whatever. 02:32 You are increasing T3,T4 in great excess, right? And from head to toe think about your patient with Graves’ disease. 02:41 Stimulates greater production of T4, lots of free T4… let me take you back to that important laboratory investigation we talked about with the resin. 02:49 “Oh Dr. Raj, don’t take me there.” Yes, I will. 02:52 So, you have increased T3, T4 and you’re increasing your total… what’s your total? Bound plus free. 02:59 You’re increasing both of these, aren’t you? Yes, you are. 03:02 In addition, you’re also increasing the amount of T3 being produced in Graves’ so you have a lot more T3 binding to your resin. 03:09 So, therefore, your T3 resin uptake will be increased. 03:12 Do you see as to how you are now utilizing and applying that information that I established earlier with laboratory investigation? Increase in T4, what’s it going to do? It’s going to suppress your TSH. 03:23 The number one screening hormone that you are going to take a look at when you’re assessing your thyroid function… TSH, TSH, TSH. 03:30 You have too much T3, T4 suppressing TSH… primary hyperthyroidism. 03:37 That increase in T3,T4 is going to speed everything up… welcome to loss of appetite, but you’re still eating perhaps, but you’re not gaining weight, that’s for sure. 03:49 Weight loss, anxiety, tremors, heat intolerance is a big one, isn’t it? Amenorrhea… you completely mess up your hormonal balance between estrogen, progesterone and LH and FSH… amenorrhea. 04:02 Graves’ disease, autoimmune disease, isn’t it? What happens to your eyes? Bulge out and you have extra ocular muscles that are undergoing hypertrophic pushing the eyes forward. 04:12 What do we call this? We call this exophthalmos… bug eyes. 04:18 Pretibial myxoedema… myxoedema is an important concept for us. 04:21 Let me now slow down here just a tad bit. 04:25 Myxoedema, you can find it in hyper; myxoedema, you can find it in hypo; myxoedema, you can find it in death. 04:34 Three different times which you’re responsible for right now in medicine with myxoedema… big time. 04:40 If it’s Graves’ disease, the myxoedema will be located… we don’t know exactly why, but you definitely will most likely find your myxoedema pretibial. 04:50 Where are you? The leg, the anterior portion, the “shin”… pretibial myxoedema. 04:56 If it’s hypothyroidism, myxoedema would be found perhaps in the hands and maybe in the face giving you the puffy hands and puffy face that you’re oh so familiar with. 05:06 And then finally, why did I say death? Worst case scenario, later on, we’ll talk about this of hypothyroidism in which the patient may actually go into a coma is called myxoedema coma and your risk of mortality increases exponentially. 05:24 Three different times in which you will find myxoedema. 05:26 I wish to make sure that you are aware where else you would find it versus just memorizing it. 05:33 Thyroid, what’s known as acropachy and thyroid bruit all because of increased amounts of T3,T4. 05:43 Now, if you have an elderly patient with hyperthyroid commonly lack these signs and symptoms. 05:51 So, therefore called “apathetic hyperthyroidism”. 05:55 Interesting enough. 05:57 If there is Grave-like issue in an elderly patient, the patient… the elderly patient is not going to behave like your typical, traditional young patient with anxiety, tremors and perhaps even loss of weight. 06:09 So, the signs and symptoms are not as prevalent, but you know for a fact that your patient has hyperthyroidism and doesn’t show you what you would expect, call this “apathetic hyperthyroidism”. 06:23 Be very, very aware of this situation because you do want to pay attention to how old your patient is whenever you have thyroid disease. 06:38 Important points of Graves’. 06:39 You’re producing thyroid stimulating immunoglobulin, autoimmune. 06:46 This is an IgG versus the TSH receptor. 06:51 Now, you tell me, are you stimulating receptor, are you inhibiting, destroying the receptor? Good, you’re stimulating… welcome to Graves’. 07:02 Autoimmune etiology, definitely want to know HLA either DR3 and B8. 07:07 If I were you, I’d memorize both of those. 07:11 More frequent in women, but you know that autoimmune diseases unfortunately generally speaking much more prevalent in the female population than male population. 07:23 Associated with exophthalmos, we talked about how you would then have autoimmune mechanism independent of hyperfunctioning Graves’ opthalmopathy… swelling of the… what is actually happening is the retroorbital muscles or extra ocular muscles are undergoing hypertrophy, you could actually see this, can be visualized on ultrasound or CT or even MRI. 07:49 It looks enlarged, pushing the orbit forward right, bug eyes. 07:56 The retroorbital fat is also increased and retro orbital swelling as you can see here in the picture beautifully illustrated. 08:04 On your left, perfectly normal, pay attention to the extra ocular retroorbital muscles normal on the left and on the right, due to excess T3,T4 undergoing hypertrophy. 08:15 Look what it’s doing. 08:16 It’s pushing the orbit forward… welcome to Graves’ opthalmopathy a.k.a exophthalmos. 08:24 With Graves’ opthalmopathy, there might be a lid retraction. 08:29 So, therefore, you find more of the orbit moving forward. 08:33 In addition to that, you will find so much of that orbit moving forward that you might actually find some of that fat that I was referring to being quite evident as you see here in the picture on the right… severe proptosis in the eye, increased vascularity of the conjunctiva, enlarged lacrimal gland. 08:54 Everything’s increased. 08:55 Take a look… take a good look as to what you can expect with Graves’. 09:00 Here, you have a shin or the pretibial region and with the symptoms of Graves’ without a doubt this is pretibial myxoedema. 09:11 What is it? It’s thickened area in the pretibial region, it appears erythematous and could extend down to the dorsum of the foot. 09:25 There might be issues with the skin. 09:27 This you would refer to as being dermopathy. 09:30 Lesions are firm, non-pitting, typically located in the pretibial region, all goes hand in hand with pretibial myxoedema. 09:39 So, you want to pay attention to, well, what exactly are they going for? Are they asking about the skin or are they asking about the pretibial myxoedema?
About the Lecture
The lecture Introduction & Graves' Disease – Hyperthyroidism (Thyrotoxicosis) by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
What is NOT a cause of hyperthyroidism?
- Radiation
- Graves' disease
- Choriocarcinoma
- Struma ovarii
- Iodine
Graves' disease is characterized by what?
- TSI acting on the TSH receptor
- Overproduction of TSH
- Overproduction of TRH
- Up-regulation of TSH receptor
- Increased deiodinase activity
Which would be expected in Graves' disease?
- TSH suppression
- TSI suppression
- TRH increase
- TSH increase
- Thyroxine suppression
Which symptom is NOT characteristically found in Graves' disease?
- Constipation
- Heat intolerance
- Pretibial myxedema
- Weight loss
- Exophthalmos
What is NOT true about the autoimmune etiology of Graves' disease?
- AIt is iodine-dependent
- Autoimmune antibody production occurs/
- There is an association with HLA-DR3/
- There is an association with diffuse toxic goiter due to autoimmune production of TSI.
- Exophthalmos can occur.
Author of lecture Introduction & Graves' Disease – Hyperthyroidism (Thyrotoxicosis)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Interesting, easy digestible lecture. Essence of useful and important information. Thanks for your work!
I finally undertood this disease which is actually nice because I couldn't associate at all with the changes in T3 and T4.
i have read the article ... it is very well explained i really ...keep up the great work
