Playlist
Show Playlist
Hide Playlist
Gastrulation and the Trilaminar Embryo

-
Slides 01-03 Gastrulation and Trilaminar Embryo.pdf
-
Download Lecture Overview
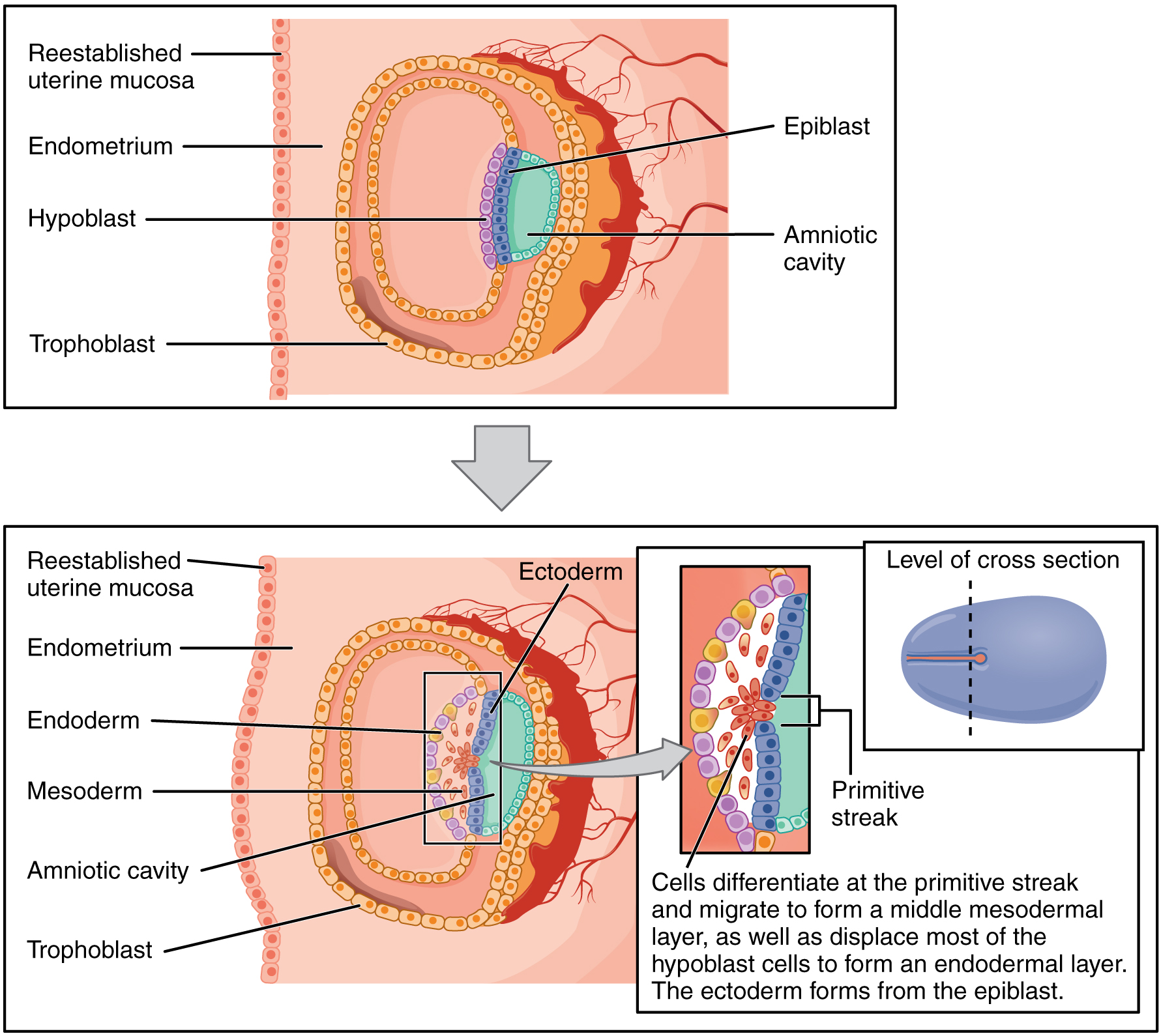
00:01 In this lecture we will discuss gastrulation, an incredibly important event in development that brings us from a bilaminar or two layered stage to the trilaminar or three layered stage. 00:12 In this process we create a series of three specific germ cell layers. 00:17 What's gonna happen here is that the epiblast of the bilaminar embryo which can create any structure in the human body subdivides into three layers the ectoderm, the endoderm, and the mesoderm and in that point, these layers have distinctive fates, things that form from ectoderm cannot form from endoderm or mesoderm and vice versa. 00:40 So these germ cell layers are gonna be the first step in very, very specialized structural formation that we're gonna follow through the rest of these lectures. 00:49 The bilaminar embryo begins the process of gastrulation by becoming polarized so there is a migration of epiblast cells from the lateral aspect toward the midline. 01:02 On the opposite side of the bilaminar embryo we development something called the primitive streak so on the more caudal side of the developing bilaminar embryo a series of cells fold inward creating a streak that moves closer and close to the prechordal plate. 01:19 At the very tip of this streak is a structure called the primitive pit and the cells that are located on the primitive pit are known as the primitive node. 01:29 As we move into this process further and further, cells are going to start folding from the epiblast down through the primitive streak and into the space underneath it. 01:42 These cells replace the hypoblast cells, creating a layer called the endoderm. 01:47 Subsequent migration through the primitive streak will form a layer in the middle, the mesoderm. 01:53 And as they continue to involute through the primitive streak and move alongside it and cranially along that space, they will utterly replace the hypoblast cells with a brand new layer called the endoderm. 02:06 The epiblast cells that did not migrate are then gonna be called the ectoderm So when all these are said and done, as the process of gastrulation completes, we have ectoderm on the top or dorsal surface of the embryo, mesoderm in the middle and endoderm lining the underside. 02:26 As we continue, a specialized set of cells are going to move through the primitive streak and primitive node and go straight towards the prechordal plate. 02:38 This specialized group of cells that are migrating directly anteriorly are called the notochordal process and they’re moving close to the prechordal plate but not quite all the way to it. 02:51 As development continues the notochordal process moves closer and closer to the prechordal plate which is also going to change names to become the oropharyngeal membrane and without too much imagination you can probably forecast that the oropharyngeal membrane will become the mouth. 03:08 On the opposite side just past the primitive streak, we have the development of the cloacal membrane which is gonna form the primordial of the anus and the urogenital systems’ openings to the outside. 03:21 We have now taken a sagittal cut through the developing trilaminar embryo. 03:26 We can see the ectoderm colored in blue, the endoderm in yellow and the mesoderm in between in red. 03:34 You can see that extending from the primitive streak closer to the prechordal plate we have the notochord and notochordal process. 03:42 As the notochordal process extends, a hollow tube forms at the center called the notochordal canal. 03:48 As it extends closer and closer to the prechordal plate, you’ll notice it never quite makes it there and the reason for that is the prechordal plate is going to become the oropharyngeal membrane and the ectoderm and the endoderm are firmly adherent to each other and will not allow mesoderm to pass between them, the same thing is happening posteriorly at the cloacal membrane. 04:11 So the firm adherence of ectoderm and endoderm marks the eventual openings of and exit from the urogenital and gastrointestinal systems. 04:21 We now have a coronal view through the trilaminar embryo. 04:25 We can see that notochordal plate is migrating in between the endoderm below and the ectoderm above. 04:33 As it’s going to form a tube, the two ends of the notochordal plate will pinch together within the mesoderm and once that happens it’s gonna pull the underlying endoderm completely together to form a continuous sheet below the notochord just as the ectoderm forms a continuous sheet above or dorsal to the notochord. 04:54 At this point the notochord is going to be a major factor in driving further development. 05:00 Now one quick preview is that the notochord only becomes the central area of our intervertebral discs and doesn’t contribute much structurally to the adult human being but during this very early stage of development the signals it releases drive the majority of important developmental sequences - they're gonna form our central nervous system and musculoskeletal system. 05:21 In particular, the ectoderm above the notochord will thicken and on either side there will be distinctive neural folds that develop and the neural groove in between the two. 05:34 Now, as mesoderm is forming and ectoderm is pulling itself in between the two layers, we're gonna get thickening and subdivision of the different regions of the mesoderm. 05:47 The portion that migrates alongside the notochord not on the exact midline but just a little bit lateral to it will flank the oropharyngeal membrane and this is the cardiogenic mesoderm, and as the name implies it will be the mesoderm that helps form the early heart. 06:05 Thereafter, mesoderm that migrates a little bit more laterally will form its specialized structures called the paraxial mesoderm, the intermediate mesoderm and lastly, the lateral plate mesoderm. 06:18 After the lateral plate mesoderm we’ve reached the point where we've met the extraembryonic mesoderm which does not contribute any tissue to the embryo itself but helps keep us connected to the umbilical cord and placenta. 06:30 Now, things that can go wrong in the process of gastrulation are many and most of them are incompatible with further life. 06:39 One set of structures that can create problem that make it to term are referred to as teratomas or monster tumors. 06:47 These are tumors that arise from the primitive streak and because they are coming from the primitive streak these overgrowths of cells, these tumors can form any structure in the human body, because the epiblast makes any structure in the body, tumors arising from the epiblast can form anything and it’s not uncommon to find partially formed limbs, hair, teeth, muscle, other structures inside these teratomas. 07:12 Most commonly, they are going to occur near the sacral coccygeal region and they're the most common neonatal tumor. 07:20 They affect females more frequently than males in a roughly four to one ratio and they are thankfully readily treated surgically and can be removed and cause no further problems. 07:31 Another very strange problem that can affect the body at this early stage of gastrulation is called primary ciliary dyskinesia and it can result in the organs of the body being completely flipped into a mirror image of their normal position, so instead of having my liver on the right side of my abdomen it could be on my left and I could have my appendix on the left side with my heart directed to the right side of my body. 07:58 This happens because as the process of gastrulation occurs, our body is deciding which side is left and which side is right. 08:07 And the reason it’s able to decide that is because a group of cells on the primitive node right on the midline where involution is occurring have cilia that beat to the left. 08:19 And as they beat to the left, they're driving a factor released by those nodal cells called nodal, so the primitive node releases the signaling molecule, nodal, and the cilia beat that singly molecule to the left which influences the cells migrating under the left side to form left sided structures and if those cilia are immobile and they do not push nodal to the left then both sides of the body receive equal amounts of it and the body has to flip a coin and determine what side is left and what side is right and then half the people with ciliary dyskinesia you will find situs inversus where the organs are flip flopped because the body flipped a coin and took the opposite route than normal. 09:07 Thank you for your attention and I’ll see you for our next talk. 09:12 Another possible defect associated with gastrulation is caudal dysgenesis. 09:17 CD is also known as sacral agenesis syndrome. It has an estimated incidence of one per 40,000 to 100,000 pregnancies. 09:28 There is agenesis of the lumbar vertebra, sacrum and coccyx with hypoplastic lower limbs and anorectal and genitourinary dysgenesis, The most likely etiology is abnormal posterior mesoderm development. 09:45 The condition is more common in offsprings of diabetic mothers.
About the Lecture
The lecture Gastrulation and the Trilaminar Embryo by Peter Ward, PhD is from the course Early Development and the Organogenic Period. It contains the following chapters:
- Gastrulation: From the Bilaminar to the Trilaminar Stage
- The Developing Trilaminar Embryo
- Defects of the Process of Gastrulation
Included Quiz Questions
What is the group of specialized cells that migrate through the primitive node towards the prechordal plate?
- Notochordal process
- Primitive streak
- Primitive pit
- Embryonic mesoderm
- Cardiogenic mesoderm
The mesoderm migrates cranially and laterally to the prechordal plate to become which of the following?
- Cardiogenic mesoderm
- Paraxial mesoderm
- Intermediate mesoderm
- Lateral plate mesoderm
- Extraembryonic mesoderm
What is the most common neonatal tumor that arises from the primitive streak?
- Teratoma
- Hemangioma
- Neuroblastoma
- Neurogenic tumor
- Lipoma
The right-left patterning of the body is influenced by what signaling molecule?
- Nodal
- EGF
- Gdf1
- Ras
- Raf
Author of lecture Gastrulation and the Trilaminar Embryo

Peter Ward, PhD
Customer reviews
3,1 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
2 |
| 1 Star |
|
3 |
This needs to be slowed down and more visual than it is.
Too fast and sometimes lacking pretty basic, though essential details about the whole process.
I find embryology confusing and this video really helped me out, thank you
One of the better lectures for this complicated subject. Images and slides are well illustrated.
