Playlist
Show Playlist
Hide Playlist
Gastroesophageal Reflux Disease (GERD): Pathology, Signs & Symptoms

-
Slides Structural GI Diseases.pdf
-
Download Lecture Overview
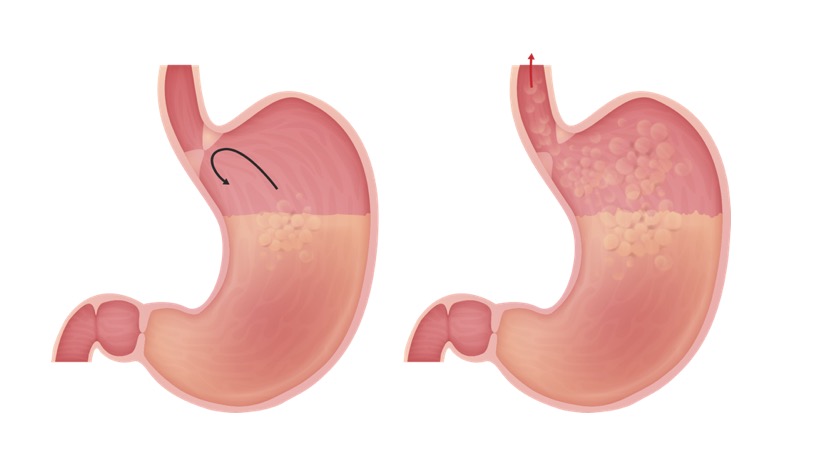
00:02 Let’s switch gears once more to a much more common problem but a disease that isn’t as common as we might think, and that’s gastroesophageal reflux disease. 00:14 So, here’s a classic example. 00:17 A nine-month-old child is presenting with frequent vomiting and poor weight gain. 00:22 This nine-month-old boy has cerebral palsy and a history of prematurity and is brought to the emergency department presenting with wheezing, stridor, and cough. 00:32 His parents are worried about his respiratory symptoms but also mentioned that his vomiting has been preventing him from gaining weight. 00:39 So, important key history points here that one would note are vomiting has been preventing from gaining weight, irritable and refusing feeds, and wheezing, stridor and cough, which remarkably, can be a sign of reflux not respiratory disease. 00:58 This is probably gastroesophageal reflux disease. 01:05 So GERD or gastroesophageal reflux disease is when stomach contents leak backward up into the esophagus. 01:14 Now, I want to distinguish this from GER, which is just gastroesophageal reflux. 01:21 Gastroesophageal reflux is a normal physiologic process in young infants. 01:29 There is not an infant in the world who has never spat up a meal. 01:33 That is normal reflux. 01:36 It becomes a disease when the child has sequelae of that disease. 01:41 So if you remember our example of our case, that child was having respiratory symptoms, was having difficulty gaining weight. 01:47 Now, it’s a disease. 01:50 Remember that 60% of infants regurgitate at least once a day. 01:55 That’s normal. 01:57 Only 5% still regurgitate at 10 to 12 months, but that’s still normal. 02:05 Five to eight percent of older children and adolescents report reflux disease symptoms such as heartburn, but only about 1% are actually treated. 02:17 So, reflux is common, disease is rare. 02:21 The key question to ask is, is this reflux causing disease or is it causing distress to the parents? The reason why that’s important is because the treatment of reflux disease has complications and risks associated with it that we have to know. 02:38 One way to distinguish this is to check the growth curves. 02:41 If you’re following those growth curves and that child is growing well, this is unlikely to be a disease. 02:47 A baby who spits up, even if they spit up every single feed and the parents swear it’s the entire feed, if that child is still growing, that child does not require a therapy. 02:59 A child who is spitting up all their feeds does not grow. 03:04 So, what causes gastroesophageal reflux disease? For reasons that are unclear, the child will have an inappropriate relaxation of the lower esophageal sphincter. 03:16 This will be exacerbated by mucosal damage of the lower esophagus from exposure to gastric acid. 03:24 It’s almost like a vicious cycle. 03:27 Also, esophageal peristalsis and the diaphragm are important in preventing reflux. 03:33 And if the child was having a problem with those muscles or those problems such as a child with nerve damage, that may exacerbate the problem. 03:41 So, risk factors for GERD include children with neurologic impairment, such as cerebral palsy or Down syndrome. 03:49 Obesity is an independent risk factor of a GERD. 03:53 Additionally, children may have esophageal anomalies such as atresia or congenital diaphragmatic hernia or achalasia, and all of those things can predispose a child to gastroesophageal reflux disease. 04:08 Children with chronic lung disease or cystic fibrosis may also be a risk for this, and premature infants are also at risk. 04:18 So historically, we need to ask the following questions. 04:21 Does this child have recurrent regurgitation or vomiting? Has the child had weight loss or poor weight gain? Those are the key questions to ask. 04:32 That’s high-yield material for your test. 04:35 Children may also be irritable. 04:37 They may have feeding refusal or anorexia. 04:41 They may have rumination. 04:43 Remember, to ruminate is not only to think, it’s also what cows do. 04:48 You can see them swallowing their cud and bringing it back up. 04:51 This can happen with children with bad reflux too. 04:54 They may actually regurgitate their meal and swallow it again. 04:58 Lastly, older children should be complaining of heartburn or chest pain around mealtime because that esophagitis will be bothersome. 05:08 In very severe cases, children may develop hematemesis. 05:12 They may have dysphagia or odynophagia, which is pain with eating. 05:18 Children with reflux disease that’s very bad, and these are usually the ones with severe cerebral palsy or other neurologic problems may also develop recurrent pneumonia as they aspirate their abdominal contents. 05:31 This can cause a recurrent wheezing and stridor as well as the upper airways are irritated by the acid that’s being aspirated. 05:41 It is important to note that gastroesophageal reflux is associated with briefly resolved unexplained events, which was what we used to call ALTE. 05:50 I’m covering this in another lecture and I would urge you to look at that lecture to fully understand this connection. 05:57 So in children with GERD, we expect to see Sandifer syndrome. 06:02 Sandifer syndrome happens in infants as they’re literally trying to escape the pain of their reflux. 06:08 You will notice children arcs their back and turn their head to their side as a way to sort of extend the esophagus to get out of the way. 06:17 If parents report that an infant is arching his back and turning his head after feeds routinely, this is probably Sandifer syndrome, and probably relates to reflux. 06:28 Patients may have pharyngeal inflammation and complain of sore throat. 06:32 And again, they may have these briefly resolved unexplained events, or they may have apnea or breath holding after feeds. 06:41 So when you’re taking a multiple choice exam, there are many findings that they will have that are clues to a diagnosis of reflux. 06:51 However, real world, we don’t see these very often. 06:56 It is in fact rare to see wheezing, coughing, stridor, or hoarseness of voice in an infant with gastroesophageal reflux, or even in children with reflux disease. 07:07 Not unheard of but not common. 07:09 The vast majority don’t have it. 07:12 Test will report children with anemia. 07:14 Again, unusual. 07:16 That’s from a chronic GI bleed, or sometimes a chronic GI bleed and not getting enough iron so they have an iron deficiency anemia. 07:25 Also, test will reveal dental erosions. 07:28 That’s almost unheard of in children but may be more common in older adults. 07:33 So, what is seen in patients with gastroesophageal reflux is esophagitis and pain, and some respiratory symptoms which may be refluxate going into an airway, and that’s really specific to those children with gross neurologic problems. 07:51 In very severe cases, children may develop failures to thrive, and they don’t want to eat and they get used to not eating and then they have a real hard time gaining weight.
About the Lecture
The lecture Gastroesophageal Reflux Disease (GERD): Pathology, Signs & Symptoms by Brian Alverson, MD is from the course Pediatric Gastroenterology. It contains the following chapters:
- GERD: Basics
- GERD: Pathology
- GERD: Signs & Symptoms
Included Quiz Questions
Approximately what percent of normal infants have symptoms of gastroesophageal reflux around 4 months of age?
- 60%
- 10%
- 20%
- 40%
- 80%
How is infantile gastroesophageal reflux (GER) different from gastroesophageal reflux disease (GERD)?
- GER is a natural phenomenon, while GERD is pathologic.
- GER refers to an episode of reflux in an infant with GERD.
- GER is forceful vomiting, while GERD is not accompanied by vomiting.
- GER is nonforceful regurgitation of food, while GERD is accompanied by forceful vomiting.
- GERD is the equivalent term for GER in adults.
Which statement below best describes Sandifer syndrome?
- Arching of the back and turning of the head after feeds
- Flexed limbs and head after feeds
- Seizures during feeds
- Generalized hypotonia on empty stomach
- Generalized hypertonia during feeds
Approximately what percentage of normal infants between 10 and 20 months of age regurgitate?
- 5%
- 15%
- 25%
- 35%
- 45%
Which of the following is requires treatment in a 3-month-old infant with gastroesophageal reflux?
- Poor weight gain
- Spitting up
- Regurgitation
- Occasional nonbilious vomiting
- Rumination
Author of lecture Gastroesophageal Reflux Disease (GERD): Pathology, Signs & Symptoms

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
