Playlist
Show Playlist
Hide Playlist
Fluid Replacement Therapy (FTP) in Children: Basics

-
Slides IVfluids Pediatrics.pdf
-
Download Lecture Overview
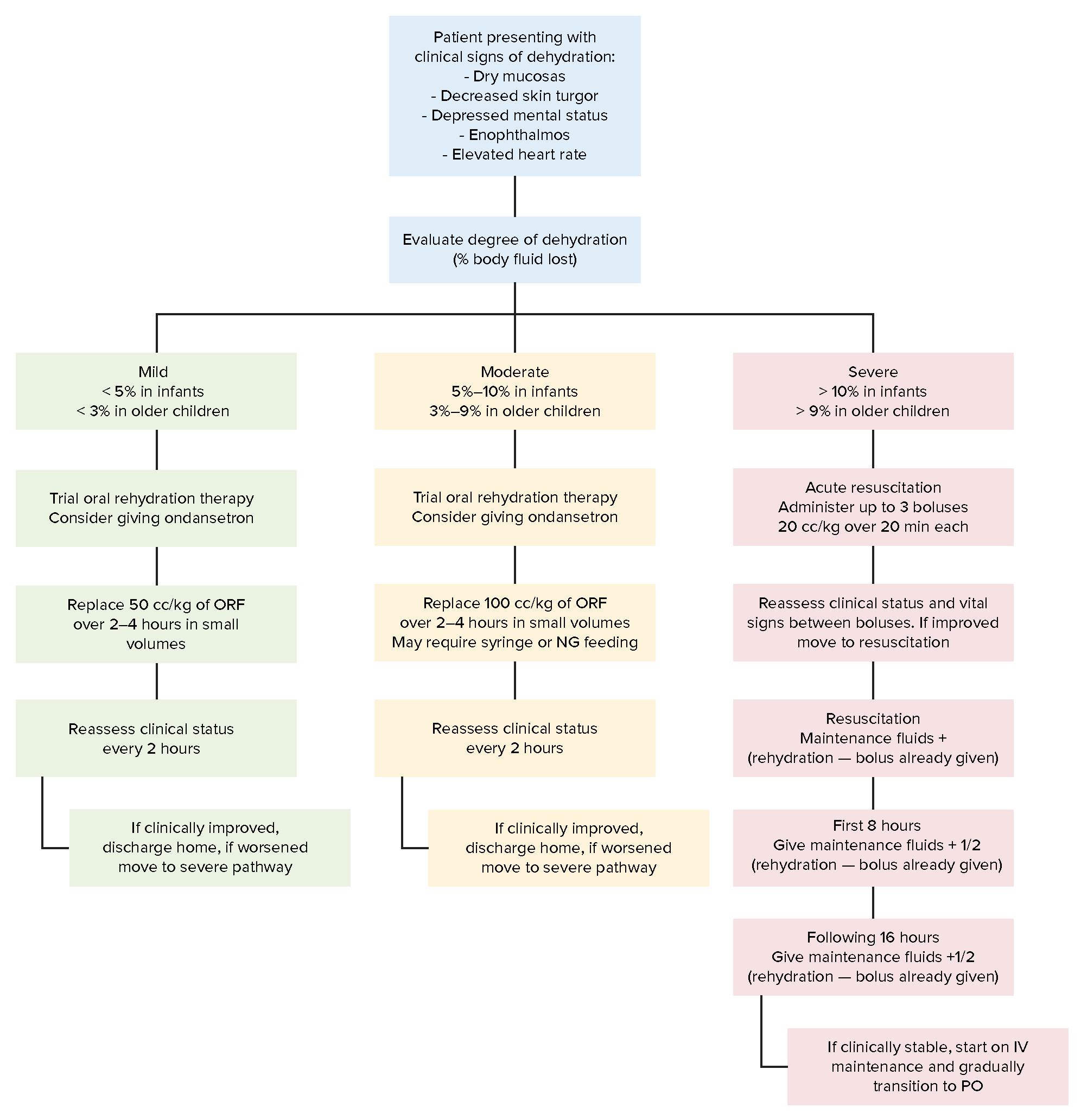
00:02 In this lecture, we’re going to discuss fluid replacement therapy in children. 00:07 This seems like a strange topic to discuss, but it turns out that fluid replacement therapy in children is a bit more complicated than in adults. 00:18 So dehydration is extremely common in children and one of the most important risks for a child’s health. 00:25 We see this all the time. 00:27 It occurs commonly in patients with upper respiratory infections like colds. 00:32 Simply they don’t want to drink. 00:34 Children with lower respiratory infections like bronchiolitis or pneumonia. 00:39 It’s common in children with vomiting from gastroenteritis for example or diarrhea, the same. 00:45 It’s also common in simply febrile illnesses. 00:48 Recall, a child has a much higher body surface area per weight than an adult does. 00:56 And so insensible losses through sweating and breathing fast are much more significant. 01:02 So when we see an infant or a child with dehydration, we want to make an assessment of exactly how dehydrated they are. 01:12 Let’s imagine three children. 01:14 A child who’s minimally, moderately, and another who is severely dehydrated. 01:19 In our minimally dehydrated child, which is about less than 3% dehydration, we really expect this child to be mostly normal. 01:29 Mental status, heart rate, mucous membranes, capillary refill, skin turgor, extremities, all of this is normal. 01:37 The first thing that becomes abnormal is a decrease in urine output. 01:41 Parents will report dry diapers or you may note decreased urine output if the patient is hospitalized. 01:48 What’s key to understand is that the kidneys holding on to fluids is the very first thing to go when a patient is minimally dehydrated. 01:59 In moderate dehydration, we see more systemic symptoms. 02:03 In particular, you’ll note a child has fatigue or irritability that may be from the illness. 02:10 Their heart rate may be increased as a way of accommodating their decreased blood volume. 02:16 What’s key is dry mucous membranes. 02:19 We see this and it’s a great way of assessing quickly whether a child is hydrated. 02:25 Also they may have fever tears present when crying. 02:29 Capillary refill may be mildly delayed around three to four seconds. 02:35 The skin turgor is still normal. 02:38 They may now have cool extremities as they’re having vasoconstriction to redirect the little blood they have where it needs to go and remember that urine output is still decreased. 02:50 As we proceed to the patient with severe dehydration, which is more than 10% dehydrated, these patients have apathy, lethargy, they do not have a normal mental status. 03:02 Heart rate will be very high. 03:04 They will have parched mucous membranes, very prolonged capillary refill and this is when you may see that tenting that you mostly read about in books or see in developing countries. 03:15 Most children don’t get that sick in the United States. 03:19 Children may have mottled extremities. 03:21 That’s from vasoconstriction of blood vessels going out to the skin. 03:26 And again, they will have almost no urine output, very decreased urine output.
About the Lecture
The lecture Fluid Replacement Therapy (FTP) in Children: Basics by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
A patient has dry mucous membranes, cool extremities, decreased urine output, and is fatigued. What would be a good estimate of his dehydration expressed in percentage?
- 5%
- 2%
- 10%
- 15%
- 20%
What is the first clinical feature that is seen in cases of minimal dehydration in children?
- Decreased urine output
- Lethargy
- Increased heart rate
- Dry mucous membrane
- Prolonged capillary refill time
Author of lecture Fluid Replacement Therapy (FTP) in Children: Basics

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very clear explanation of what are the hallmarks of the three degrees of dehydration
