Playlist
Show Playlist
Hide Playlist
Failure to Thrive (FTT): Pathology

-
Slides FailuretoThrive Pediatrics.pdf
-
Download Lecture Overview
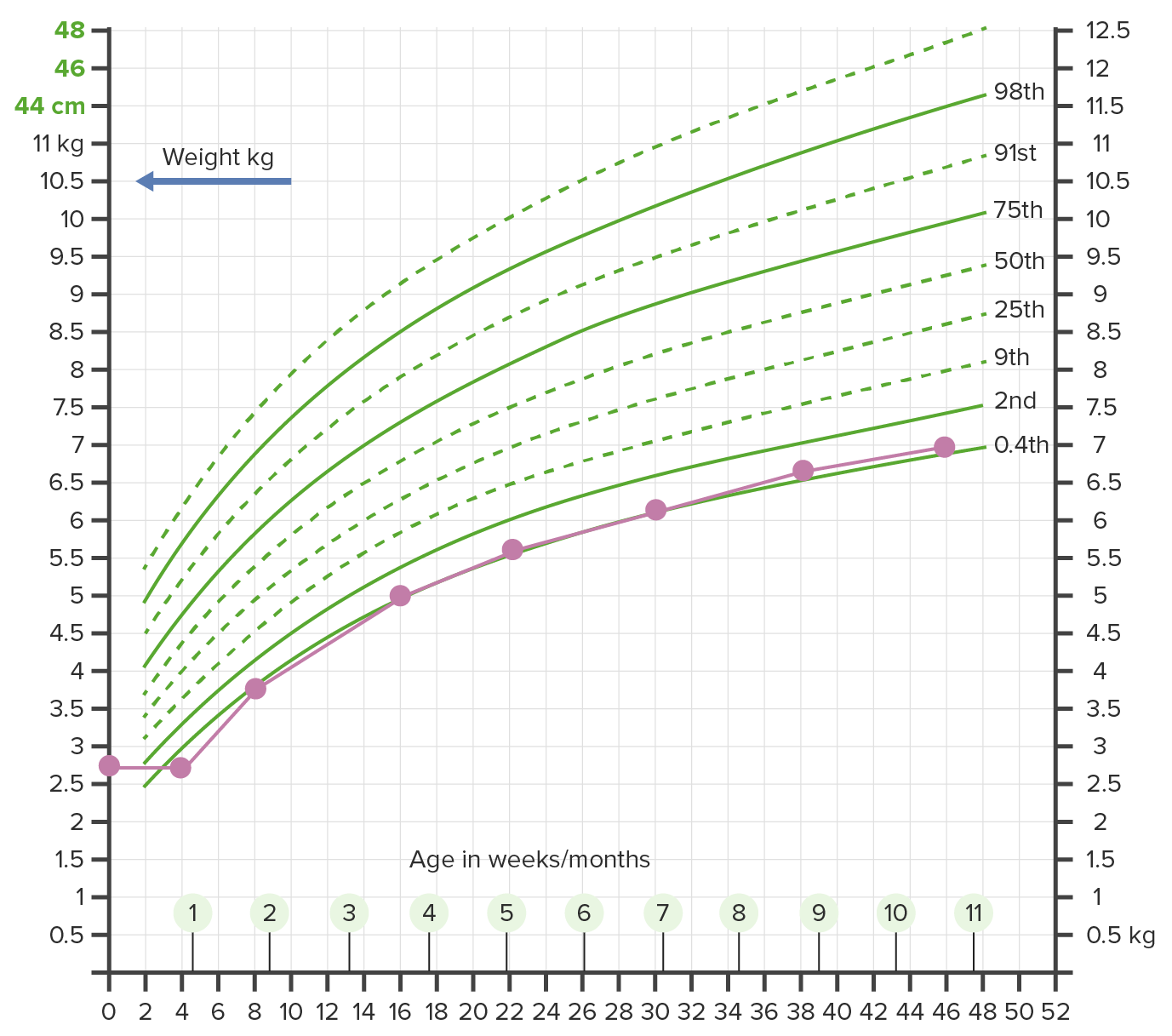
00:02 In this lecture, we will discuss failure to thrive in the infant. 00:08 Failure to thrive is sub-optimal weight gain and growth in infants and toddlers when compared to peers on standardized growth charts. 00:18 There are many causes to failure to thrive, and there may be multiple factors that are affecting a child’s inability to grow. 00:27 This can be medical or they can be psychosocial. 00:32 When we suspect failure to thrive, we will typically plot children on a growth curve, as you can see here. 00:38 And we’ll have another lecture on growth curves and how we watch these children. 00:43 But typically, failure to thrive is when we see weight below the second percentile for age and gender on more than one occasion. 00:53 Typically, we will expect to see a weight of less than 80% than what is ideal for that age. 01:01 And we also call failure to thrive when children are dropping off their growth curve, for example, more than two major percentage lines in a six-month period. 01:13 When you look at these two charts here, you can see two children who are growing. 01:19 On the middle of this slide, we can see a child who started off at a reasonable weight after birth, and then has been tracking appropriately below the line. 01:29 This child may not have failure to thrive even though we’re seeing multiple points below the second percentile because this child is continuing to track at that percentile. 01:42 Chances are this child may have a genetic syndrome or something else that’s causing to not grow well. 01:48 This is a patient we would be concerned about and will work up for a failure to thrive, but we may eventually just accept this is where this child is going to be. 01:57 On the flipside, on the far end of this slide, we can see a child who was born in a particular weight which is a little bit higher, and then it’s tracking along a percentile that is reasonably appropriate. 02:10 That child likely does not have failure to thrive. 02:14 So what are the causes of failure to thrive? There are many, and let’s break them down to large groups. 02:21 So in the first group, we have inadequate intake or absorption of calories. 02:27 So if a child is not absorbing or is not taking enough calories, they’re not going to grow, or it’s possible a child might have inefficient or defective ability to use those calories, or a child may have excessive metabolic demands. 02:43 Let’s look at all these three categories individually. 02:47 So for inadequate intake or absorption, there are many potential causes of failure to thrive. 02:53 There can be non-organic or environmental causes and there can be organic causes. 02:58 First, let’s look at non-organic causes. 03:01 Certainly, a lack of available food or child abuse or neglect are high in the list. 03:06 In fact, child neglect is by far and away the number one cause of infants who have failure to thrive. 03:15 Psychosocial deprivation or not paying attention to a child may cause a child to not want to eat, and that may in turn reduce the amount of available calories. 03:27 In the organic list, some children may have an impaired ability to suck or swallow, which is hampering their ability to absorb calories. 03:35 They may have a chronic illness, which is making them not have much hunger or drive to eat. 03:41 In the inadequate retention department, we think of children who have excessive vomiting or children with very severe gastro-esophageal reflux. 03:52 Keep in mind especially with gastro-esophageal reflux that these are the children we’re going to treat for reflux. 03:58 We don’t treat children for reflux typically, unless they’re having problems with weight gain. 04:06 Children may have malabsorption. 04:08 In other words, they can’t absorb the calories that they're otherwise eating adequately. 04:13 There are few diseases that can cause this. 04:16 One might be celiac disease. 04:18 Celiac disease is an autoimmune response to gluten in the diet, which blunts the ability of that intestine to absorb calories. 04:27 Cystic fibrosis patients frequently have malabsorption as a result of pancreatic insufficiency. 04:33 Patients with milk protein intolerance when still unrecognized may have an allergic reaction in their intestinal wall, which is preventing them from adequately gaining calories. 04:45 Children with necrotizing enterocolitis in the newborn period, especially premature children, may have sections of intestine removed as a surgical option to prevent them from dying of NEC. 04:59 Those children then have a short gut for the rest of their lives and may have problems absorbing calories. 05:05 So children with short gut syndrome may present with failure to thrive. 05:11 There are other categories where children are adequately getting the nutrients but they just can’t utilize them correctly. 05:18 There are some syndromes such as chromosomal abnormalities where children can’t utilize their nutrition. 05:26 Children with severe prematurity or IUGR, intrauterine growth restriction, may have a problem utilizing appropriate nutrition. 05:35 Certainly, children with metabolic disorders will have a problem utilizing nutrients. 05:40 If I have a problem breaking down proteins and digesting them, I might not be able to get those calories. 05:48 Another example in the metabolic contingency would be congenital hypothyroidism. 05:53 These children have a hard time growing. 05:56 Children with congenital infections may have a harder time utilizing nutrients maybe through hepatic failure or other reasons like that. 06:04 And certainly, children with storage disorders will have problems. 06:08 Lastly, children with metabolic diseases like amino acid or organic acid disorders may have problems utilizing appropriate nutrition. 06:18 Some patients may be able to eat and use nutrients appropriately, but simply have such high metabolic demands that they aren’t able to keep up with their body’s own needs. 06:30 These children will have a hard time growing. 06:33 Examples would be a patient with thyrotoxicosis where the revved-up body’s metabolic demands are too high for what a child can catch up with. 06:43 This is all so true of patients with cystic fibrosis or respiratory effort might require more metabolic requirements. 06:51 Malignancies are classic. 06:52 So, weight loss in malignancy is not uncommon. 06:56 Patients with chronic infections may have a problem keeping up with their body’s metabolic demands. 07:01 An example would be HIV. 07:04 Children with immunodeficiency are especially prone to getting chronic infections, and these children sometimes have problems gaining weight as well. 07:12 Congenital heart disease commonly presents with failure to thrive. 07:15 In fact, that may be the presenting symptom. 07:18 And likewise, again, children with amino acid and organic acid disorders also have increased metabolic requirements, which drive some of their failure to thrive.
About the Lecture
The lecture Failure to Thrive (FTT): Pathology by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
What is the most common medical cause for failure to thrive in infants?
- Hypothyroidism
- Celiac disease
- Cystic fibrosis
- Milk protein allergy
- Metabolic diseases
A 3-year-old boy with failure to thrive is brought to a pediatrician who suspects malabsorption might be the cause. Which of the following is NOT a cause of failure to thrive in children due to malabsorption?
- Inflammatory bowel disease
- Cystic fibrosis
- Milk protein intolerance
- Short gut syndrome
- Celiac disease
Increased metabolic demand may lead to failure to thrive. Which of the following is NOT a cause of increased metabolic demand in children?
- Celiac disease
- Malignancy
- Thyrotoxicosis
- Chronic infection
- Cystic fibrosis
Failure to Thrive is primarily calibrated by which of the following parameters?
- Weight
- Age
- Height
- Activity
- Sleep
Author of lecture Failure to Thrive (FTT): Pathology

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good lecture, I would have appreciated more details on the differential diagnosis. Very clear explanations, though! Thanks!
