Playlist
Show Playlist
Hide Playlist
Failure to Thrive (FTT): Management

-
Slides FailuretoThrive Pediatrics.pdf
-
Download Lecture Overview
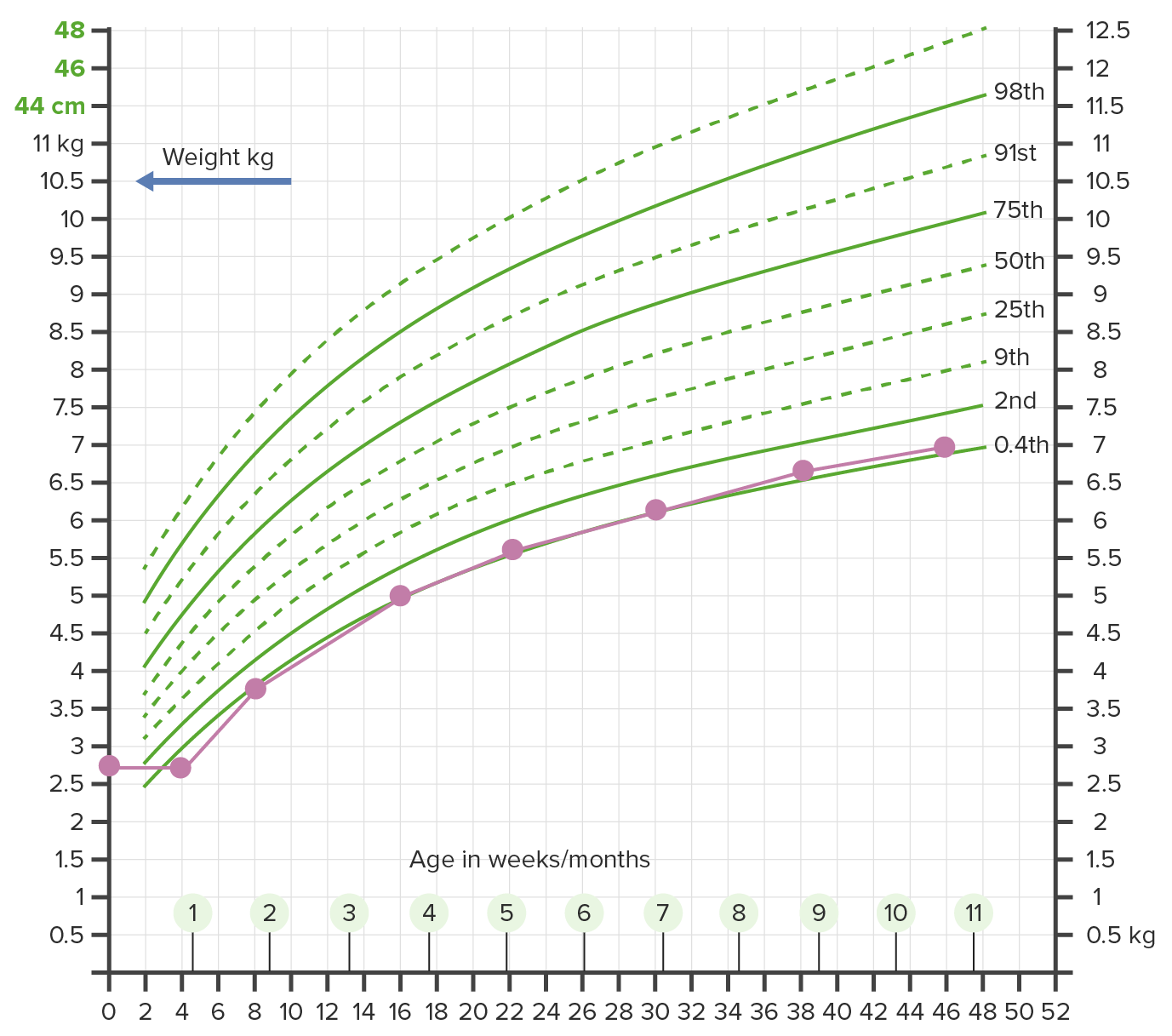
00:02 So how do we manage these children with non-organic failure to thrive? This is the majority of these children. 00:10 We certainly support positive eating behavior. 00:13 We try to encourage a positive eating environment for these children and their families. 00:18 We will engage a pediatric dietician to come and assess how much is this child eating and what is this child eating and how can we boost calories. 00:30 And these dieticians may recommend strategies to increase energy intake. 00:35 I’ll give you a few examples. 00:37 In the younger infants, sometimes we’ll concentrate the formula. 00:41 Normal formula is 20 kcal per ounce. 00:44 We might boost that to 22, 24, 27 or very rarely 30 kcal per ounce to try and increase the amount of calories the child is eating without giving the child increased effort to actually just take in more calories. 01:01 In older children, sometimes we’ll supplement food into their diet. 01:05 And by that I mean sprinkle in extra fat, sprinkle in some extra protein. 01:10 There are lots of clever ways we can actually sneak extra calories into children’s food. 01:17 Oftentimes, a clinical psychologist or social services are warranted to try and help the family deal with whatever are the stressors that are causing them to neglect their child. 01:28 A child abuse specialist consult is indicated if we suspect child abuse or child neglect. 01:34 It can be incredibly helpful in not only making the diagnosis and engaging in a discussion with the family that is appropriate for a court of law, but also they can help us in terms of followup with these children if there’s no followup available in the community. 01:51 Typically, we only admit children six months of age because we want to track growth very carefully or in children who have severe failure to thrive and have a concern for refeeding syndrome. 02:07 Refeeding syndrome is an unusual problem in these children, but let’s review it briefly. 02:13 As you recall, in people who have significant starvation, if we refeed them too quickly, they have large pools of ADP. 02:24 They can make their ATP because they have no sugar. 02:28 As a result, when they are acutely refed, the ADP is rapidly transferred into ATP, driving down their serum phosphate levels and a very low serum phosphate level is a potential risk for sudden death. 02:44 So we don’t want to refeed children who have been starving very quickly. 02:50 We want to do it slowly. 02:51 And this is often done in a supervised setting. 02:55 So what are the outcomes? The outcomes are tricky especially in these children with social failure to thrive because some of those outcomes are a result of being brought up in a dysfunctional environment. 03:10 However, what we often see in these children who don’t eat well early in life is a continued undereating throughout life. 03:18 Sometimes parents can be very frustrated with this. 03:20 They just can’t get their kids to eat as much as they want. 03:24 But also, sometimes parent don’t quite understand what the expectations of their child’s growth are. 03:32 Remember, at the start of our lecture, we looked a couple of children who are growing appropriately at a very low level of the curve. 03:38 If that’s where that child is, sometimes parent get frustrated because they can’t get their child to a percentile that’s really than where that child is going to go. 03:48 These children will typically remain underweight and they may have some short-term impaired development as they’re untreated until they are treated. 03:59 An example would be often in children or infants with failure to thrive, there’s a delay in rolling over, sitting up or standing or walking or talking, but once they’re fed, they rapidly catch up. 04:12 If children are untreated, they are at risk for short stature. 04:17 They’re at risk for secondary immune deficiencies because if you don’t have much protein, it’s harder to make antibodies and they are gravely at risk for long-term cognitive and behavioral problems as they grow into young adults. 04:35 So this is our classic case, we have a two-year-old male who’s not growing. 04:41 His parents are going through a divorce and begin arguing in the office and they’re asked to leave the room. 04:47 The nurse assesses the child’s height and weight and the pediatrician immediately is worried, noticing that this child has not changed in weight from the last visit, which was already low. 05:01 There’s stress in this family, this child is not changing in his height and weight for the last few visits and now is below the second percentile. 05:13 What are the facts of this that are concerning? Well, certainly this child is now below the second percentile and probably we have a few measurements that are corroborating this fact. 05:25 Remember, one low level may just be an abnormal scale. 05:31 Notice it’s from the last visit, which was already low. 05:36 Additionally, we can here his parents are going through a divorce and begin arguing in the office and are asked to leave the room. 05:43 This is probably a sign that this child has a social cause of failure to thrive. 05:50 This is a classic example of what we might see in the office. 05:54 Thanks for your attention.
About the Lecture
The lecture Failure to Thrive (FTT): Management by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
Which is NOT a typical consequence of untreated non-organic failure to thrive?
- Hypoglycemia
- Short stature
- Secondary immune deficiency
- Cognitive delay
- Behavioral problems
Refeeding syndrome may lead to death by which of the following mechanisms?
- Very low phosphate levels
- Very low potassium levels
- Low insulin levels
- Very low glucose levels
- Very high lipid levels
What is the normal per ounce caloric value of standard formula milk?
- 20kcal
- 15kcal
- 30kcal
- 35kcal
- 40kcal
Author of lecture Failure to Thrive (FTT): Management

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great lecture for one of THE pediatric topics. It addresses all the important aspects of the topic.
