Playlist
Show Playlist
Hide Playlist
Etiology and Diagnostics – Rheumatic Heart Disease


-
Slides Valvular Hypertensive Heart Disease.pdf
-
Download Lecture Overview
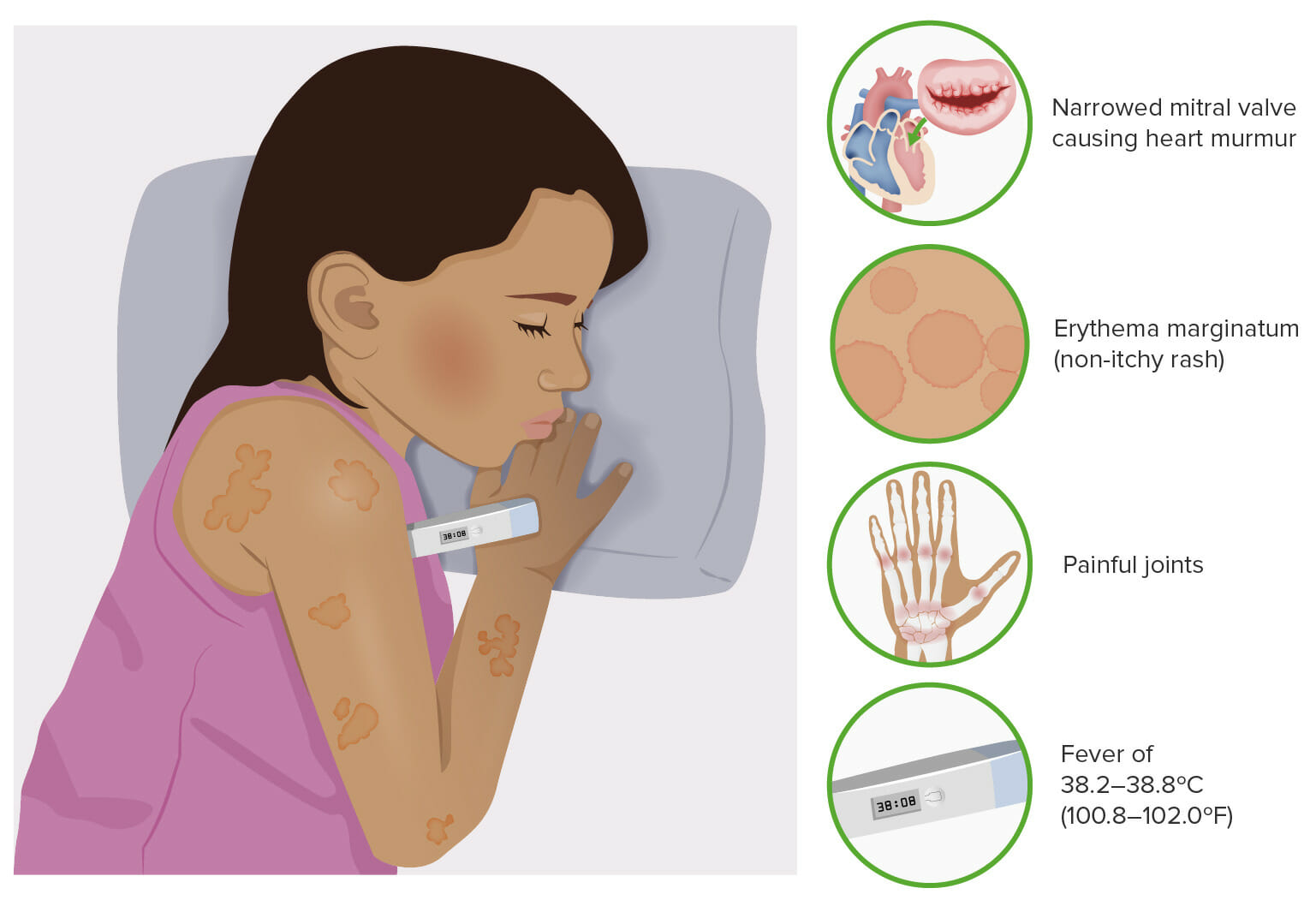
00:01 <b>Let's talk about another etiology for valvular disease.</b> <b>This is rheumatic fever. A rheumatic fever, as you are </b> <b>probably abundantly aware,</b> <b>is an acute immunologically mediated multisystem </b> <b>inflammatory disease</b> <b>that typically begins, classically, a few weeks after a </b> <b>group A streptococcal pharyngitis.</b> <b>So, we're looking into the pharynx of this person,</b> <b>and we have some angry read mucosa, and we have some </b> <b>enlarged nodes</b> <b>and, in this case, would be due to streptococcus </b> <b>pharyngitis.</b> <b>The immune response to the strep bacteria</b> <b>as we will see in the next couple of slides gives rise to </b> <b>auto - to antibodies that,</b> <b>for good or for ill in some patients, recognize or </b> <b>cross-recognize heart antigens,</b> <b>and that will be the cause of the valvular disease.</b> <b>You can also have those same antibodies and some of the </b> <b>inflammatory T cells</b> <b>can also cause myocarditis or a pericarditis.</b> <b>So, the systemic manifestations, when you are developing </b> <b>immune response</b> <b>to the streptococcal bacteria that caused the pharyngitis,</b> <b>you can have other manifestations that are part of acute </b> <b>rheumatic fever. Okay?</b> <b>It's not just the valvular disease or the carditis that </b> <b>affects the heart,</b> <b>you - classically, there are five kind of Jones criteria,</b> <b>five major manifestations that you need to be thinking </b> <b>about.</b> <b>The first one there is subcutaneous nodules typically on </b> <b>extensor surfaces of the elbows and the knees.</b> <b>Erythema marginatum which is an irregular kind of somewhat </b> <b>circular rash</b> <b>that can be on any body surface.</b> <b>Sydenham's chorea, this is due to immune complex deposition</b> <b>or antibodies binding to particular antigens in various </b> <b>parts of the basal ganglia</b> <b>and you get patients with kind of uncontrollable </b> <b>choreoathetoid movements.</b> <b>There's a polyarthritis. Again, probably immune complex </b> <b>and/or direct antibody binding.</b> <b>So, you get a polyarthritis.</b> <b>And the Jones criteria means that we have evidence of a </b> <b>preceding group A streptococcal infection,</b> <b>and then a certain number of the major or minor criteria.</b> <b>So, on the previous slide were the major criteria.</b> <b>And then, we have minor criteria that include things</b> <b>like fever, arthralgia, elevated blood levels of acute phase</b> <b> reactants.</b> <b>So, already mentioned this several times,</b> <b>but now you've heard it probably for the third time, so it's</b> <b> maybe important.</b> <b>It does show up on the boards.</b> <b> About 85% of the time, Rheumatic heart disease is the cause</b> <b> of mitral stenosis.</b> <b>And here, you see the valve is thickened, it is somewhat </b> <b>stenotic,</b> <b>and the atrium behind it is quite dilated</b> <b>as a result of the increased pressure having to go through </b> <b>that tight valve.</b> <b>The epidemiology of this. So, in developed countries, this </b> <b>is not a major problem.</b> <b>That's because we improved sanitation, less streptococcal </b> <b>distribution within the population,</b> <b>and also because we have very rapid diagnosis in treatment </b> <b>of strep pharyngitis</b> <b>so that we treat with antibiotics before patients develop </b> <b>any significant antibody titer.</b> <b>So, overall, in the US, many places in Europe,</b> <b>there's a declining incidence in mortality from rheumatic </b> <b>fever and rheumatic heart disease.</b> <b>On the other hand, in developing countries,</b> <b>it's still an important public health problem estimated at </b> <b>15 million people a year</b> <b>who have some degree of rheumatic heart disease.</b>
About the Lecture
The lecture Etiology and Diagnostics – Rheumatic Heart Disease by Richard Mitchell, MD, PhD is from the course Valvular and Hypertensive Heart Disease.
Included Quiz Questions
What pathogen is likely responsible for mitral regurgitation in a patient who develops symptoms four weeks after an upper respiratory infection with pharyngitis?
- Group A streptococcus
- Staph aureus
- Staph epidermidis
- Group B streptococcus
- Coxsackievirus
Which of the following is NOT a systemic manifestation of acute rheumatic fever?
- Splinter hemorrhages
- Circular rash (erythema marginatum)
- Uncontrollable movements (Sydenham chorea)
- Subcutaneous nodules on extensor surfaces
- Polyarthritis
What is the correct definition of the Jones criteria for the initial diagnosis of rheumatic fever, in addition to evidence of prior group A streptococcal infection?
- 2 major manifestations OR 1 major + 2 minor manifestations
- 2 major manifestations only
- 1 major + 2 minor manifestations only
- 3 major + 1 minor manifestations
- 1 major OR 2 minor manifestations
Author of lecture Etiology and Diagnostics – Rheumatic Heart Disease

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
