Playlist
Show Playlist
Hide Playlist
Elbow Anatomy: Nerves and Diagnosis of Radial Head Dysfunction

-
Slides Ostepathic Diagnosis of the Elbow Region.pdf
-
Download Lecture Overview
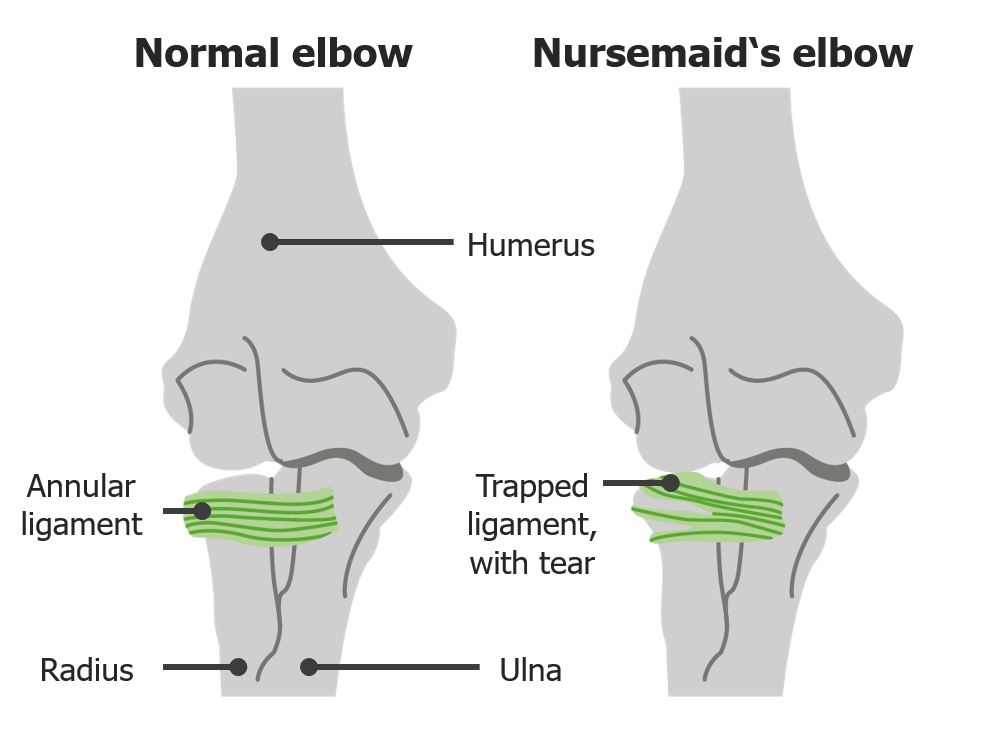
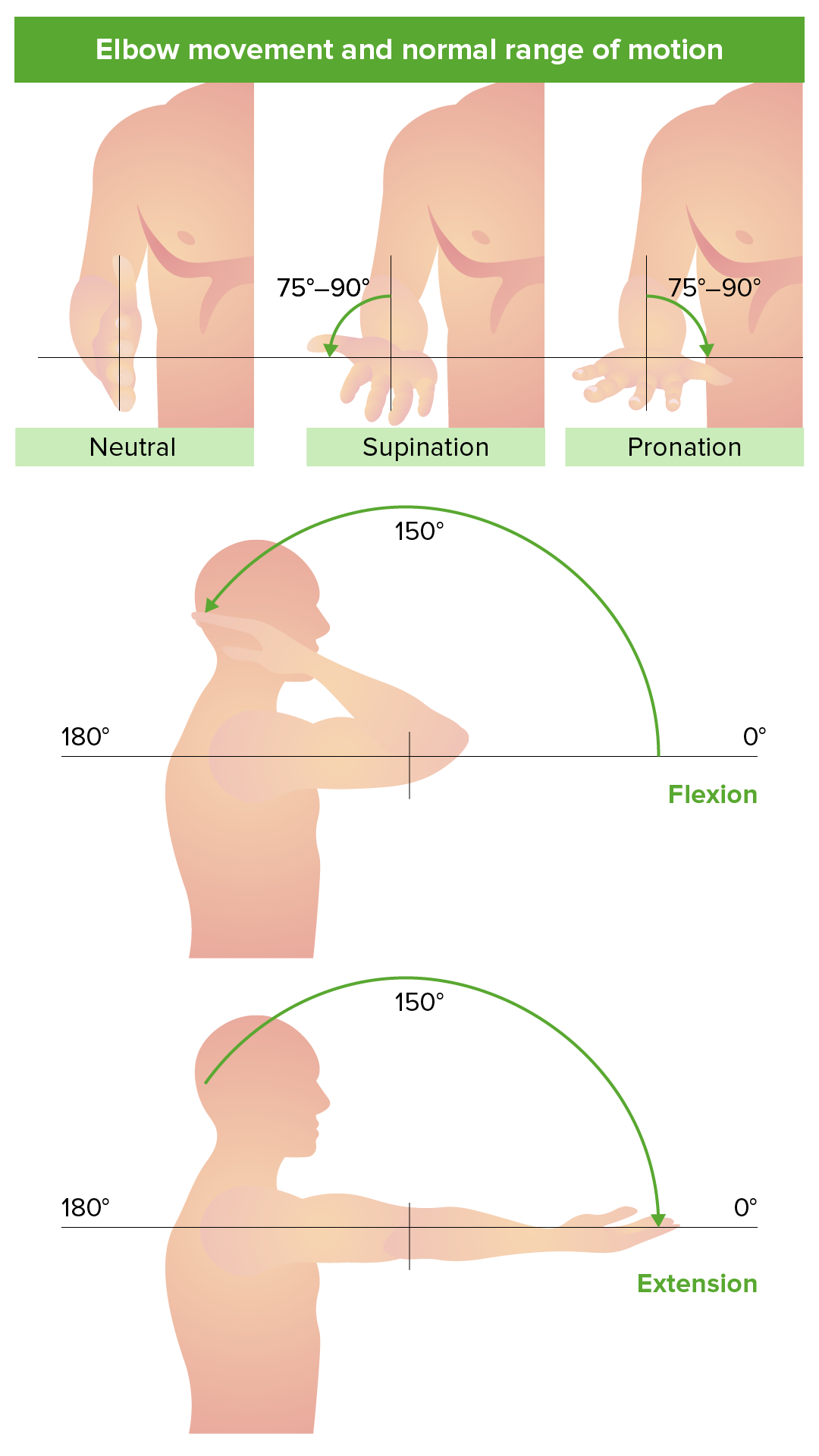
00:01 So it's important to really understand the nerves that pass through the elbow understanding the location of the nerves to give you a better idea on when the might be impinged. 00:10 Patients that complain about certain weaknesses, numbness and tingling of the hand or the forearm or radiating pain could potentially have nerve compression and so understanding the route of these nerves are important to better understand where they may be potentially compressed. 00:25 So the median nerve lies deep to the antecubital fossa, it is medial to the biceps brachii. 00:32 The radial nerve is lateral to the biceps and brachialis muscle. 00:37 whereas the ulnar nerve runs more posteriorly and posterior to the medial epicondyle running through the ulnar groove. 00:45 So the ulnar nerve innervates the ulnar collateral ligaments and supplies the flexor carpi ulnaris The median nerve passes between the brachialis and the bicipital aponeurosis to supply the pronator muscles and most of the wrist and hand flexors. 01:01 The radial nerve has a medial and posterior branch that supplies the triceps, anconeus and the posterior and anteriolateral joint capsule. 01:09 They also have a lateral branch that pierces the lateral intermuscular septum and that supplies brachialis, brachioradialis, extensor carpi radialis longus and also continues on as the posterior interosseous nerve. 01:25 So somatic dysfunctions can occur at the elbow joint. 01:28 These dysfunctions could be due to injury or repetitive motion. 01:32 Most of the time it's associated with some sort of inflammation and muscle spasms and sometimes would be compensation for injuries outside of the elbow, at the wrist or shoulder. 01:42 So when we're trying to diagnose a somatic dysfunction we're making it based on motion testing. 01:47 And so, if we have a restriction in flexion or extension, that could lead us to make a diagnosis of a flexion or extension dysfunction. 01:56 So remember, somatic dysfunctions are named for its freedom. 01:59 So if I have a flexion dysfunction of the elbow, that means that there's a preference for flexion and that there's a limited range of motion in extension. 02:07 The opposite is true in an extension dysfunction The elbow prefers extension but then has difficulty reaching the full range of motion in flexion. 02:16 At the radial ulnar joint, we have pronation and supination as motions. 02:21 If we have restrictions in a pronation or supination, that could lead us to diagnosing somatic dysfunctions in that motion. 02:28 So if I have a pronation somatic dysfunction, we're gonna have a restriction in supination because pronation is the freedom of motion. 02:36 Now, there's an association between the radial head positioning and how the forearm likes to glide. 02:43 So, a radial head that is stuck in a posterior position prefers pronation whereas a supination dysfunction has restriction in pronation and the radilal head is not going to prefer anterior glide. 03:00 So another way to diagnose radial head somatic dysfunction specifically is to contact the radial head and then motion test. 03:09 So when we motion test, what we're going to do is we're going to passively move the forearm into supination and pronation and while we're monitoring at the radial head, we're gonna see which way does the movement of the radial head feel freer Does the radial head move more posterior in pronation or does it move more anterior in supination? So that is one way to passively test freedom of motion at the radial head. 03:33 An alternative way is to do an active screening. 03:36 So in an active screening, we're gonna have our patients kinda put their elbows against their body and have their elbows flexed at 90 degrees. 03:44 We're gonna start at neutral and then we're gonna ask the patients to pronate both sides and supinate both sides. 03:51 And so what you're looking for, is there a freedom of motion to either pronation or supination as the patient does that. 03:58 The diagnosis is made with the side of increased freedom. 04:03 An easy way to remember the direction of motion of the radial head with pronation and supination is a mnemonic PPAS, 'cause if you'll remember it, it'll help you pass your examinations. 04:13 So, P-P-A-S. 04:14 Posterior is associated with pronation and anterior radial head is associated with supination. 04:21 So let's apply the knowledge that we just covered. 04:24 A 45 year old tennis player presents with right lateral elbow pain. 04:27 On active range of motion testing you find that he is only able to pronate his right elbow about 5 degrees while having full range of motion with supination. 04:35 What is his radial head somatic dysfunction diagnosis? So here, we have the tennis player who is unable to fully pronate his elbow. 04:49 So if you are unable to fully pronate your elbow, you have a freedom of motion in supination. 04:54 Remember back that we have the radial head is more anterior, that's associated with supination while posterior is associated with pronation. 05:02 So in this case, we have a right anterior radial head somatic dysfunction. 05:07 This is a case where we have a 14-year old male presents with right elbow pain after tripping and falling 2 days ago. 05:13 He states that he fell forward on his right wrist with his elbow extended. 05:17 X-rays of the elbow were negative for fracture and on passive motion testing, there was a decreased in right elbow supination. 05:23 So what is the radial head somatic dysfunction? So here, our patient fell with outreached hand forward. 05:34 And so, what you notice here is that the forearm is pronated, we have a crossing of the ulna and radius. 05:40 So when you fall forward and land on your wrist, a lot of times that jams the radius into the elbow and creates a dysfunction. 05:47 If it's crossed over, then it's more posterior because our forearm is pronated. 05:52 and so that would lead to an increased risk of a posterior radial head dysfunction. 05:56 The motion and characteristics on testing also confirmed that since there was decreased right elbow supination, the freedom of motion was pronation. 06:05 Thus, giving us our diagnosis of a posterior radial head The opposite would be true if we were to fall with hand behind us because our forearm is now straight and where our forearm is supinated, when we jam the elbow in a supinated position that might cause anterior radial head.
About the Lecture
The lecture Elbow Anatomy: Nerves and Diagnosis of Radial Head Dysfunction by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Elbow Region. It contains the following chapters:
- Anatomy: Nerves
- Radial Head Dysfunction Diagnosis
Included Quiz Questions
Through which of the following structures does the radial nerve pass before eventually continuing as the posterior interosseous nerve?
- Intermuscular septum
- Extensor carpi radialis longus
- Pronator muscle
- Cubital fossa
- Brachioradialis
Which of the following movements occurs primarily at the radioulnar joints?
- Pronation and supination
- Extension and rotation
- Flexion and extension
- Medio-lateral rotation
- Antero-posterior glide
During normal movements of the elbow, which of the following motions causes the radial head to move posteriorly?
- Pronation
- Supination
- Flexion
- Extension
- Retraction
A 30-year-old woman with diabetes comes to the outpatient department with complaints of inability to completely supinate her hand while flipping pancakes. What is the most likely somatic dysfunction?
- Somatic dysfunction - posterior radial head
- Somatic dysfunction - anterior radial head
- Somatic dysfunction - lateral radial head
- Somatic dysfunction - medial radial head
Author of lecture Elbow Anatomy: Nerves and Diagnosis of Radial Head Dysfunction

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Superb way of showing anatomical parts with a greate deal of errort
