Playlist
Show Playlist
Hide Playlist
Dizziness

-
Slides Dizziness AcuteCare.pdf
-
Download Lecture Overview
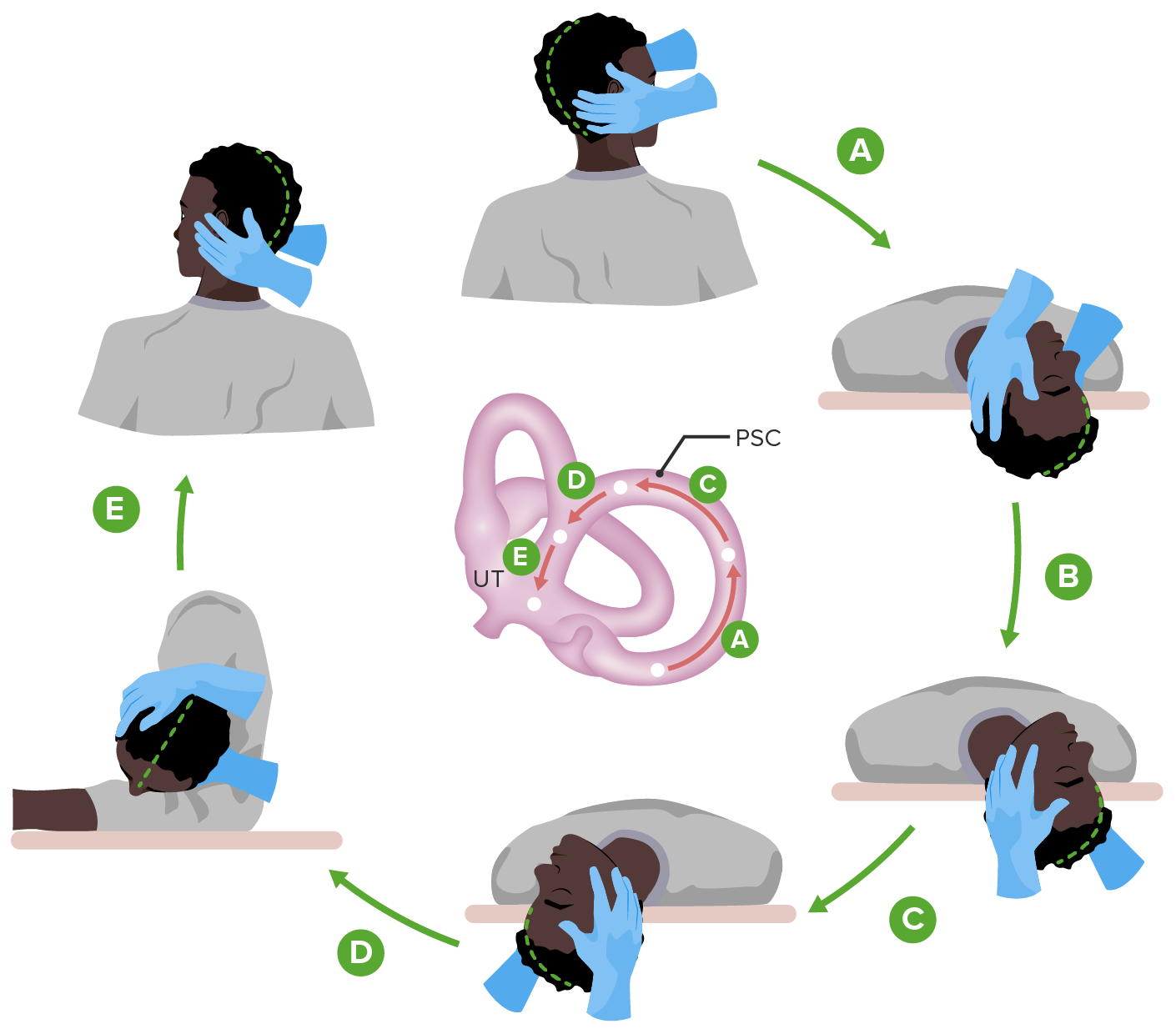
00:01 So, a lot of providers dislike seeing patients with dizziness. 00:05 It can be a difficult condition to diagnose. 00:09 But I'm going to try to give you some pearls today that help guide you through the diagnosis and the management of patients with dizziness. 00:17 So, hopefully, you really embrace it. 00:18 And if you do, you’ll become very popular in your practice and get a lot more dizziness patients sent your way. 00:23 Trust me. 00:25 So, this is a pretty extreme example of feeling dizzy. 00:30 Just looking at it makes me a little bit dizzy. 00:32 But there have been some broad studies that look at the types of symptoms that patients complain of when they’re talking about dizziness because it’s not just one disorder. 00:41 We’re talking about different diagnoses and even different symptoms. 00:45 So, half of cases involve vertigo, in which the patient actually feels the room spinning around. 00:52 And another 25% just feel lightheaded, at disequilibrium. 00:58 And that’s actually interesting to me because it's more, in my practice, the reverse, but in large epidemiologic studies vertigo is more common. 01:05 Pre-syncope, feeling like you’re going to faint, up to 14%, and then the rest is other. 01:11 So, here's what I do. 01:12 One is I really try to get down to what exact symptom do patients feel. 01:18 And it really comes down to disequilibrium versus vertigo. 01:23 And when I say don't be afraid to show the patient, actually I asked them, do you feel like the room is spinning around like this or do you just feel like you're really unsteady on your feet. 01:35 And I feel like, if I just explain it without pantomiming the symptom to the patient, they'll get a little confused. 01:42 But when I show them, whoa, disequilibrium or, whoa, vertigo, they’ll just point and say that one. 01:50 That's the one I have. 01:52 And that's going to take you down two different roads in terms of diagnosis. 01:58 So, one thing that’s important as well, think hard about the medications the patient is on, drugs that are sedating, antihypertensive drugs, any drug that lowers blood pressure, anticholinergic drugs, all of these are associated with dizziness as well. 02:11 So, think about what you may be prescribing and the harm it may be having on patients. 02:16 Another nice dividing line is hearing loss. 02:19 If they do have hearing loss, think about labyrinthitis or Ménière's disease. 02:25 If they don't have hearing loss and they have vertigo specifically, could be benign positional vertigo or vestibular neuritis situation. 02:35 Other things you should think about when evaluating patients with dizziness, do they have anxiety? Is there a lot of stress in their lives? Palpitations could be a sign of arrhythmia, patients with atrial fibrillation will often have some dizziness because their cardiac output is decreased overall. 02:53 And substance use. 02:54 Any time that patients who are either using or withdrawing from substances, they may feel dizzy as well. 03:03 So, some important parts of the physical exam, your physical exam is going to play a role here. 03:08 Do consider getting orthostatic pressure and pulse levels. 03:11 See if it changes between lying down to sitting to standing with your patients. 03:19 And Dix-Hallpike maneuver is a great test for benign positional vertigo. 03:24 It has a decent sensitivity overall and this is where you have the patient's head and you have them go from a sitting position to a lying position with their head down to one side in a rather swift maneuver. 03:37 If they have symptoms of vertigo, and particularly if they’re have a nystagmus at the same time, it's a positive testing and you can feel comfortable that they have benign positional vertigo. 03:49 Every patient with dizziness deserves some neurological evaluation. 03:53 I do the cranial nerves on all these patients. 03:55 I’ll check a Romberg study for cerebellar function. 03:58 I’ll look at their gait, which measures a bunch of different functions together. 04:02 And then I'm going to listen to their heart, make sure they're not in arrhythmia. 04:06 I’ll listen to their carotids too, particularly in an older patient, maybe a critical carotid stenosis is contributing to that dizziness, the lack of blood flow to the brain. 04:17 Workup, it's easy to go wild and order all kinds of head imaging studies and esoteric lab studies. 04:26 Certainly, you can have metabolic conditions that contribute to dizziness as well. 04:31 But I want to be just focused as much as possible. 04:36 I check for anemia, check for thyroid function, check a BMP for any gross electrolyte abnormalities or maybe a really high glucose and previously undiagnosed diabetes. 04:47 But that's really it. 04:48 And I try not to reorder these tests on a frequent basis. 04:52 Sure, two years later, that dizzy patient may have developed thyroid disease or anemia, but what really frustrates me is when patients have this checked every three or four months as if something is really going to change. 05:03 They’re just dizzy. 05:04 Neuroimaging is not usually necessary. 05:07 If your history and your physical suggests one of these more benign forms of dizziness, don't get extra imaging. 05:16 It’s just extra radiation the patient does not need and won't further your diagnosis along. 05:23 Benign positional vertigo, the most common cause of vertigo, simple maneuvers which I usually provide handouts to patient on how to do. 05:32 They can be done in the office. 05:34 Oftentimes, it might need to be repeated at home, but it is remarkable in that they can be effective in just one or two tries of doing the Epley maneuver, which is basically rotating your head in such a way that's moving the debris out of the semicircular canals, which is promoting the vertigo in the first place. 05:52 But patients can do this once or three times and are cured, which is remarkable. 05:58 Much better than giving drugs over time because drugs like meclizine, they can be effective for the vertigo, but they mostly do so by causing sedation and they can make you a little bit – feeling of a disequilibrium as well. 06:13 In terms of Ménière's disease, that’s a different disorder. 06:16 There you’re going to restrict salt, use diuretics such as triamterene/hydrochlorothiazide are good for the acute attacks of Ménière's disease. 06:25 And those patients all often have them see an ENT specialist. 06:29 Same with vestibular neuritis. 06:31 More rare, but the recommended treatment does include a corticosteroid tapered over three weeks. 06:40 So, that gives you some insight into vertigo specifically and some of the causative reasons that people get dizzy, but I would recommend doing that separation, showing your patient the different forms of dizziness and making sure that they understand disequilibrium and vertigo are usually separate events, and then that will help guide your diagnostic process from there. 07:03 Don't overuse labs either. 07:05 And then recommend things like Epley maneuver for patients as first-line treatment for benign positional vertigo. 07:12 Thanks very much.
About the Lecture
The lecture Dizziness by Charles Vega, MD is from the course Acute Care. It contains the following chapters:
- Dizziness
- Important Parts of Physical Exam
- Management of Dizziness
Included Quiz Questions
Which of the following tests for canalithiasis of the posterior semicircular canal in benign paroxysmal positional vertigo?
- Dix-Hallpike maneuver
- Carotid auscultation
- Head impulse test
- Ocular tilt reaction
- Head-shaking visual acuity
Which of the following is the most appropriate initial therapy in a patient with benign paroxysmal positional vertigo and a positive Dix-Hallpike maneuver?
- Epley maneuver
- Meclizine
- Salt restriction
- Hydrochlorothiazide
- Methylprednisolone
Which of the following best defines disequilibrium?
- A sense of imbalance that occurs primarily when walking.
- An illusion of motion
- The prodromal symptom of fainting or a near faint
- Ataxia of gait
- Dizziness that commonly results in an altered level of consciousness
Which of the following is the classic triad of Meniere's disease?
- Episodic vertigo, tinnitus, hearing loss
- Headache, episodic vertigo, tinnitus
- Episodic vertigo, tinnitus, vomiting
- Headache, ataxia, vomiting
- Headache, hearing loss, vomiting
Which of the following is the most appropriate initial therapy for Meniere's disease?
- Salt restriction
- Epley maneuver
- Methylprednisolone
- Nonsteroidal anti-inflammatory drugs
- Meclizine
Author of lecture Dizziness

Charles Vega, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
