Playlist
Show Playlist
Hide Playlist
Diarrhea: Etiology

-
Slides GIP Diarrhea.pdf
-
Download Lecture Overview
00:01 Welcome. If you've been looking at the various talks associated with gastrointestinal pathology, you knew that this one was coming. Let's talk about diarrhea. 00:11 So, in many cases, we have in our own mind what definition we would use for diarrhea. 00:19 There is a formal one that we recognize and it's greater than three loose or watery stools within a 24-hour period. 00:28 The etiology is incredibly broad and once you start thinking about the ways that the GI tract might malfunction, you can pretty much explain diarrhea in a hundred different ways. 00:44 But I'm - we're going to try to give you here a way to think about diarrhea. 00:48 So, it can be, and it is, basically, an increased frequency and there's not solid stools. 00:56 There may or may not be cramping or blood, or mucus, or fat, or flatus. 01:02 Those will tend to indicate various causes. But it's just the increased frequency. 01:08 We can break it down into acute, usually, self-limited. Persistent, that would go on for days to weeks. 01:16 And chronic, forever. There are many causes. So, it can be infectious. 01:21 It can be primarily predominantly inflammatory. It can be toxic, it can be surgical, so, iatrogenic. 01:28 Can be due to increased motility. Again, there are a variety of ways that diarrhea can occur. 01:34 So, another way to kind of parse this out is to think about where is the abnormality occurring? Is it in the small bowel? Is it in the large bowel? And this will have different manifestations but will also have different import as we'll talk about. 01:52 So, in the small bowel disease, that's where we absorb nutrition and that's where we're getting all of our vitamins and our basic fat absorption and amino acids and electrolytes. 02:05 So, if there is a small bowel disease, that diarrhea's going to be associated with vitamin deficiency and malnutrition. 02:12 There's frequently going to be an associated steatorrhea. We're not absorbing fats. 02:18 You're going to have voluminous, floating, greasy, foul-smelling stools. 02:23 And it's mainly, the main manifestations of this are all going to be malabsorption. 02:29 On the other hand, if we have large bowel disease, things involving the colon, we're going to have a different set of problems. 02:38 The colon is where we largely absorb water and failure or pathology associated with large bowel diseases can lead to dehydration. 02:47 We'll have increased water and electrolyte loss that goes with that into the stool. 02:55 Another way to parse this out, so, we've talked about acute and persistent, and chronic. 02:59 We've talked about things that involve the small bowel and the large bowel. 03:02 Now, let's talk about the underlying causes. So, infectious diarrhea. 03:06 And some infections induce an inflammatory response and it's a combination of the bug and the inflammation that we would get diarrhea. In other infectious diarrheas, it's not inflammatory. 03:18 These tend to be infections that release an exotoxin that cause a secretory diarrhea and we'll talk about that in a moment. 03:28 Amongst the inflammatory diarrheas that are infectious, bacteria, so, Shigella, Salmonella, Campylobacter. 03:37 and various protozoans as you see there can be causal. 03:41 In the non-inflammatory infectious diarrheas, this is because of the elaboration often of toxins. 03:49 So, of the bacterial varieties, enterotoxigenic E. Coli, Tropheryma whipplei, not necessarily making a toxin but by causing macrophage expansion, we're not getting good absorption. 04:03 Vibrio cholera does elaborate a toxin. Talk about that in a moment. 04:08 Viral causes may include rotavirus and adenovirus. 04:11 Amongst the Protozoans that can cause a non-inflammatory diarrhea, Giardia, really common, Cyclospora, Cryptosporidia, Isospora. 04:24 So, if it's going to be infectious, it's probably coming from the outside world. 04:30 So, contaminated food, contaminated water, association with critters, animal exposures, are all going to be kind of risk factors for developing infectious inflammatory injury within the GI tract. 04:45 There are also certain high-risk environments. 04:48 So, daycare facilities with little kids sharing all the nasty little bugs that the little kids get. 04:53 Nursing homes and hospitals are also high-risk environments for the passage of infectious agents. 05:00 If patients are immunocompromised, don't have the normal inflammatory or immune response to organisms that - the GI tract, that also puts particular subset of people at risk. 05:15 Traveler's diarrhea is a very common entity and we've talked about it in another talk within the series. 05:21 It occurs in about 40% to 60%. So roughly, half of the travelers that go to a developing country. 05:27 And these are typically bacterial, enterotoxigenic E. coli, Campylobacter jejuni, Shigella, and Salmonella species are all potential agents depending on what part of the world you're in. 05:40 Pseudomembranous colitis. This is specific entity. So, it's diarrhea in a setting of prior antibiotic administration. 05:48 And what happens is that you take an antibiotic, say, for an ear infection or for a throat infection, or for a urinary tract infection, that antibiotic clears that infection but then, also kills off the normal host microbiota, the microflora. 06:05 In many cases, the antibiotics that we're taking for an otitis or a pharyngitis or a cystitis, those don't necessarily kill off all the organisms. 06:16 And you may have then, a residual population that are not killed by the antibiotic and that overgrow. 06:23 And in particular, in a subset of the human population walking around out there, they have a small population of an organism, Clostridioides difficile, a gram positive rod. 06:36 And patients or individuals who take antibiotics with that population may get now an overexpansion. 06:44 Well, the Clostrioides difficile when they're in small numbers don't usually cause a problem. 06:49 But when they are the predominant species within the GI tract, they cause problems by the elaboration of a toxin. 06:57 And that toxin will actually kill epithelial cells and you will lose the normal epithelial barrier and you will have malabsorption. 07:05 So, in thinking again about kind of categories of diarrhea. 07:10 Infectious diarrhea can be inflammatory or non-inflammatory. 07:14 We've covered that. Now, we're going to talk about non-infectious diarrhea. 07:18 And it can be secretory, osmotic, associated with malabsorption, or inflammatory. 07:27 Of the non-infectious diarrheas, secretory, for example, can be due to laxatives and primary laxative abuse. 07:34 Factitious diarrhea is something one should always consider with people who keep coming back with the same sort of problem. 07:43 Osmotic or malabsorptive diarrhea can happen with entities such as lactose intolerance and celiac disease. 07:50 And I'm not going to go into excruciating detail here, but if you want to, those are separate talks within this GI pathophysiology series. 07:58 We can have inflammatory or exudative non-infectious diarrhea. 08:02 This is going to be the inflammatory bowel diseases such as Crohn's Disease and Ulcerative Colitis. 08:07 And again, we will talk about those in some detail in separate talks within the series. 08:12 And then, you can have altered motility. Think about it. 08:15 If your bowel's just going from top to bottom, then, you are not going to have enough time to absorb what you need to absorb even if everything else is perfect. 08:25 So, irritable bowel syndrome and hyperthyroidism by driving increased intestinal motility can also be a cause of a non-infectious diarrhea. 08:34 So, I had mentioned factitious diarrhea. Interestingly, epidemiologically speaking, greater than 90% of cases are in women, often associated with healthcare workers who can understand the mechanisms by which they can take certain agents and have a diarrhea and they get secondary benefit from people being - wanting to be helpful to them. 08:59 These individuals are so called frequent flyers. They will have frequent hospital admissions for the same entity. 09:06 They'll come to the hospital, we'll be able to monitor their activities. The diarrhea will go away. 09:11 We will have done an entire workup, not been able to find it, and they go home. 09:16 And then, for whatever psychologic reason, they will then reappear, be readmitted with new diarrhea caused again by the same agent, laxatives. 09:30 So, laxative abuse can occur. Individuals may think that they are - they need to continue to take laxatives even after they've had constipation resolved and that will lead to a diarrhea, clearly. 09:47 And then, we have individuals who have anorexia nervosa or bulimia who take laxatives as part of that underlying psychological kind of substrate. 09:57 So, long discussion about etiologies. 10:01 But hopefully, we have now a way of thinking and compartmentalizing various forms of diarrhea.
About the Lecture
The lecture Diarrhea: Etiology by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
What is the definition of "diarrhea"?
- Three or more watery or loose stools in a 24-hour period
- Four or more watery or loose stools in a 24-hour period
- Five or more watery or loose stools in a 24-hour period
- Five or more stringlike stools in a 24-hour period
- Four or more stringlike stools in a 24-hour period
What is the key feature of diarrhea?
- Increased bowel frequency
- Abdominal cramping
- Blood in the stool
- Mucus in the stool
- Increased flatus
What is one effect that diarrhea from small bowel disease can have that is NOT usually present in diarrhea from large bowel disease?
- Vitamin deficiency
- Dehydration
- Reduced water uptake
- Increased water loss
- Electrolyte loss
What is a risk factor for infectious diarrhea?
- Animal exposure
- CDKN2A mutation
- Arsenic exposure
- Radon exposure
- RET mutation
Author of lecture Diarrhea: Etiology

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
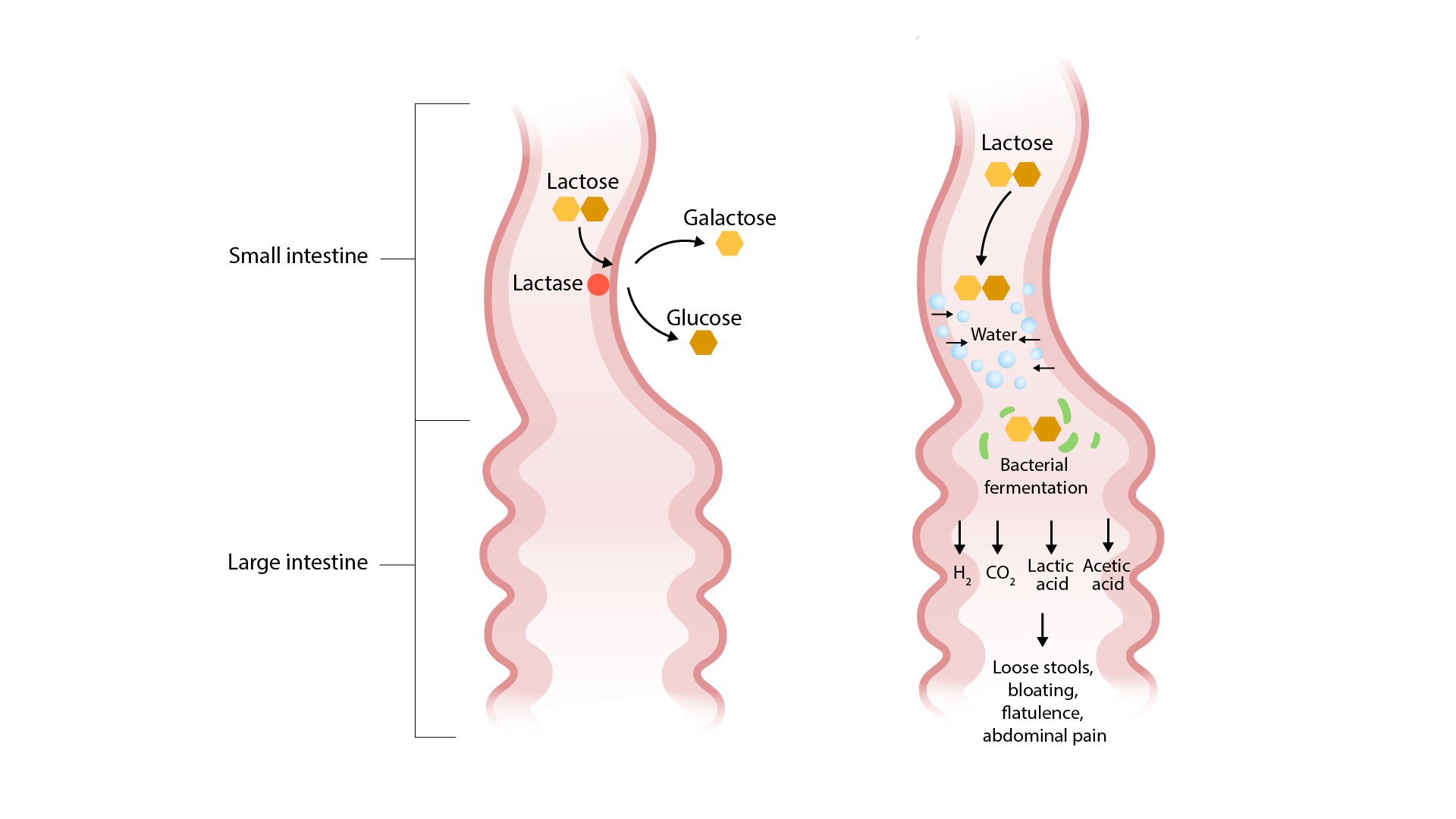
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
