Playlist
Show Playlist
Hide Playlist
Control of Growth Hormone Release


-
Slides AnteriorPituirary EndocrinePathology.pdf
-
Download Lecture Overview
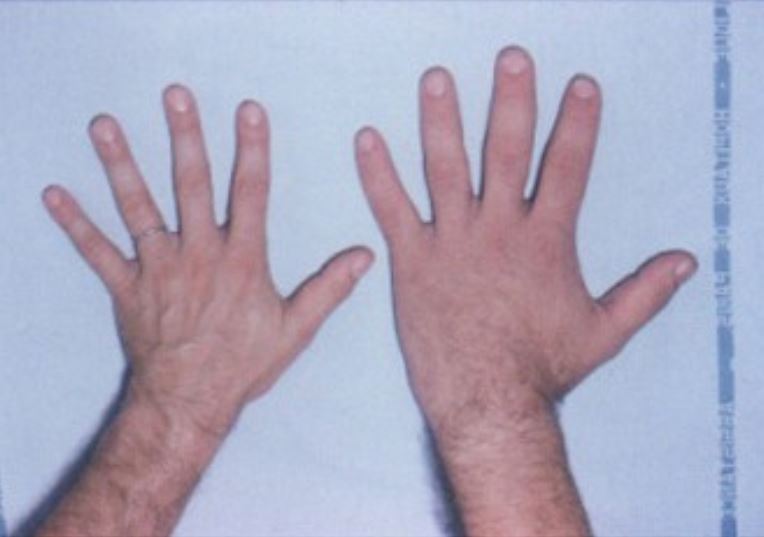
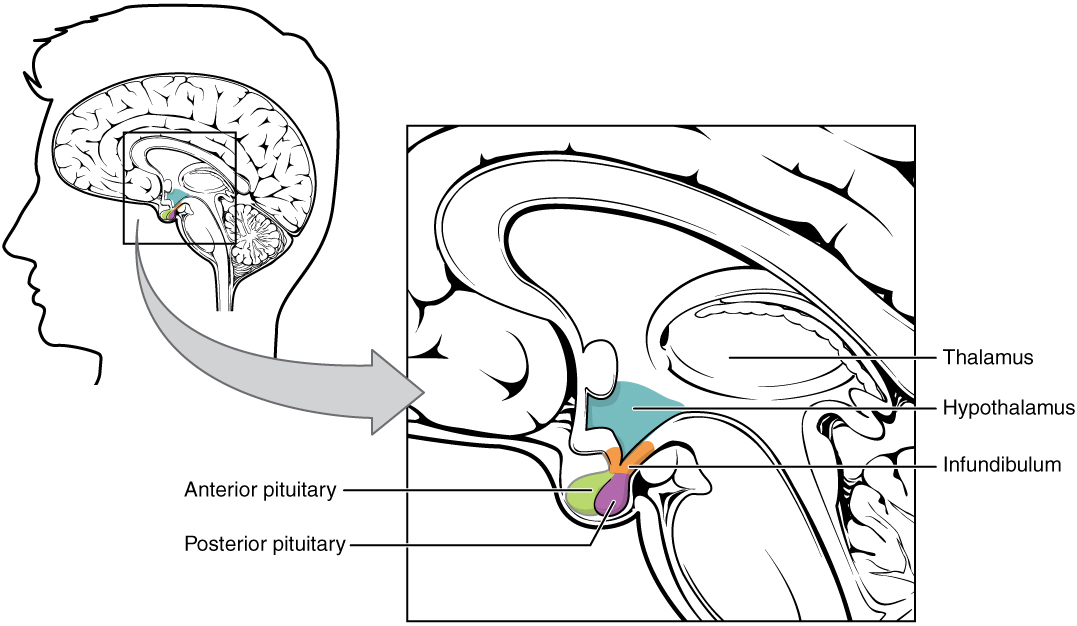
00:01 Let’s now move on to growth hormone. 00:04 Growth hormone, a couple of things here. 00:07 The way that this is setup is the following. 00:09 We’ll begin with the hypothalamus with our releasing hormone/inhibiting hormone. 00:14 We’ll move from the hypothalamus into the anterior pituitary. 00:19 This is then known as your somatotroph. 00:22 Collectively, remember that growth hormone LH share a common precursor known as somatommamotropin and growth hormone will be released from the anterior pituitary, works upon the liver where it then releases your insulin-like growth factor. 00:40 On your left, you’ll notice the following. 00:43 Remember that growth hormone is something that’s released more so at night when one is sleeping. 00:49 So, therefore, that pulsatile nature making growth hormone measurement not the most reliable and also, the growth hormone is a stress hormone. 01:01 With that said, please look at the stimuli on your left. 01:04 We have sleep… big time; exercise… when you exercise, you’re consuming glucose. 01:12 Hypoglycaemia, amino acids… all of these will be triggers for the hypothalamus to release growth hormone releasing hormone. 01:22 On the other side of things, we have growth hormone inhibiting hormone. 01:25 Please take a look at the key over to your far right and you’ll notice somatostatin. 01:30 Once again I reiterate that growth hormone inhibiting hormone is also called somatostatin. 01:36 Used to be called, once upon a time, just to make sure we cover all basis, that insulin-like growth factor was called somatomedin. 01:42 So, there are lot of terms here that have the prefix somato-, somato-, somato-… somatostatin, somtatotroph, somatomedin… mediating your growth hormone. 01:54 Next ,we are going to travel through our portal circulation. 01:56 By that, we mean what? From the hypothalamus through this stalk, through portal vein and we’re entering the anterior pituitary. 02:06 Within the anterior pituitary, what is the name of the cell and what stain is it that releases growth hormone? The name of the cell is somatotroph, it stains pink or acidophil. 02:22 It’s responsible for releasing growth hormone. 02:27 This will then work upon the liver. 02:30 From the liver, we release our insulin-like growth factor and this insulin-like growth factor is going to be responsible for the vast, vast functioning of our growth hormone including during a child when we’re growing up into puberty, our linear growth of our long bones. 02:50 Keep in mind that the inhibitory or the feedback mechanism for IGF1 which is the most important measurement laboratory wise of how well our growth hormone is functioning in our body has a stimulatory effect on your somatostatin. 03:11 Secretion of growth hormone by somatotroph is regulated by… we talked about growth hormone releasing hormone and somatostatin a.k.a. growth hormone inhibiting hormone. 03:23 If excessive growth hormone is being secreted, then as a child, we or the child becomes a giant or gigantism as an adult. 03:36 And if it’s an adult that has excess growth hormone, obviously referred to as your acromegaly. 03:43 Here, we have excess amounts of somatomedins are formed by growth hormone coming from the liver. 03:52 It’s important that you know that somatomedin exhibits or exerts its inhibitory effect on your growth hormone by stimulating somatostatin. 04:03 Negative feedback signals are overridden during sleep when growth hormone levels are highest. 04:10 That is important for you to take out of this section. 04:14 Hence, the pulsatile nature and the fact that growth hormone has a shorter half-life than IGF1 making it a less reliable laboratory indicator. 04:28 The target organ is the following. 04:30 Let me set this up… of the growth hormone IGF1 combination. 04:37 The combination of the two or each separately has different effects, as we shall see. 04:44 Let’s begin. 04:46 Target hypothalamus releasing your growth hormone releasing hormone works in the anterior pituitary releasing growth hormone, out comes the growth hormone. 04:54 The growth hormone has a couple of things. 04:56 Remember, this is stress hormone. 04:58 So, therefore, you are then going to breakdown your lipid… lipolysis hence releasing your free fatty acids. 05:05 You are also going to release your ketones from your muscle, you’re going to release glucose. 05:11 Remember what are we doing here? We are making sure that we do everything in our power to take those cells that are going to give us the precursors for gluconeogenesis biochemically, aren’t we, and for protein synthesis. 05:25 So, it’s going to take all of this from our adipocytes, our liver and muscle and then place it into circulation, hence the green tube that you see here. 05:37 The green tube represents the circulation and from the circulation, you’ll notice here the somatomedin means what? Insulin-like growth factor, coming from where? The liver, is then responsible for growth. 05:53 It’s responsible for linear growth of your long bones, as you see here; it’s responsible for protein synthesis, as you can see here; and to build everything up of your viscera. 06:10 Everything is growing and this is mostly due to the effect of IGF1, insulin-like growth factor. 06:19 Here, it’s showing you growth hormone working up upon your adipocytes resulting in lipolysis. 06:32 Here, from the liver growth hormone works through gluconeogenesis being the biochemical pathway. 06:42 Growth hormone from the liver is going to release insulin-like growth factor 1. 06:48 From the muscle, remember, it wants to have or bring in those amino acids, it’s the precursor uptake protein synthesis by growth hormone and IGF. 07:01 Here, through the action of IGF, you will have linear bone growth, you’ll have protein synthesis and you have a visceral maturity. 07:12 All of these would be through the actions of somatomedin. 07:15 Prior to all these was the effect of growth hormone on different cells and tissues… adipocytes, muscles cells and liver. 07:25 Somatomedin, bone growth, on your viscera… growth. 07:34 Without any of this, we have the following issues. 07:37 In the middle, we have a normal child at the age of approximately 13. 07:43 On your left is a patient who doesn’t have growth hormone and this is what’s called as Lorain levi. 07:54 On your right, you also find a suboptimal patient with a growth hormone and this is called Frohlich’s dwarf. 08:03 Of all the three patients and of the two that have growth hormone dysfunction, you’ll notice that Lorain levi are those patients that seem to be the or have the shortest defect or the shortest growth. 08:19 So, what’s happening here with Lorain levi? It’s the fact that there’s an actual problem within your growth hormone receptor. 08:28 If the receptors do not ever function, then what do you know about the precursor hormone or the hormone prior? It’s always elevated. 08:38 Deficiency or absence of somatotroph cells, underproduction of growth hormone, delayed skeletal growth and retarded sexual development, but alert, intelligent, well proportional child. 08:51 IQ perfectly okay, however as far as growth is concerned, it is completely retarded. 08:59 Now, when you have Frohlich… in Frohlich, the problem is the following. 09:06 A destructive disease of part of the anterior pituitary and usually with damage to posterior pituitary as well and that usually will help you a little bit more. 09:15 There’s going to be decreased production of growth hormone and because the anterior pituitary might be affected during development; if the thyroid hormones have been affected, there’s going to be the most important statement here apart from the fact that there’s going to be stunting of growth and mental-mental sub-normal or sub-optimal mental activity. 09:42 We did not see this with Lorain levi type of growth hormone dysfunction. 09:48 Obesity and large appetite for sugar; if atrophy of other endocrine glands, signs of deficiency of their hormone. 09:55 So, with Frohlich, you’re thinking about your anti-pituitary being more of an issue; with Lorain levi, you’re thinking more about your growth hormone receptor being an issue. 10:06 Know growth hormone in great detail. 10:09 What if it was growth hormone excess? As a kid, there’s gigantism, pretty straight-forward… long bones over grow as epiphyseal plates are yet diffused. 10:20 As an adult, known as acromegaly, there might be soft tissue growth, there will be visceromegaly. 10:26 There might be prognathism, the jaw that I talked about being extremely pronounced and increased cardiovascular mortality with reduced life expectancy in non-cured individuals. 10:38 Because there’s visceromegaly as well, “Hey doc, my hat size is increasing.” Now, with that said, that gives you a couple differentials, I’ll just name a few. 10:47 Sure, it could be acromegaly, it could also be Paget’s disease of the bone or it could be something like osteopetrosis. 10:55 Okay, so, the three major complaints or-or the expression of hat size increasing once again would be acromegaly and Paget’s disease of the bone. 11:08 Those are the two big ones, then we’ll get into orthopaedics, we’ll talk about Paget’s disease of the bone further so that you clearly distinguish acromegaly from this and the other one technically that might also have increased hat size includes osteopetrosis.
About the Lecture
The lecture Control of Growth Hormone Release by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
Which statement about the synthesis of insulin-like growth factor 1 (IGF-1) is most accurate?
- It is stimulated by growth hormone in the liver.
- It is stimulated by growth hormone-releasing hormone in the anterior pituitary.
- It is stimulated by growth hormone-releasing hormone in the liver.
- It is stimulated by growth hormone in the anterior pituitary.
- It is stimulated by growth hormone-releasing hormone in the hypothalamus.
What increases growth hormone secretion?
- Growth hormone-releasing hormone
- Somatostatin
- Somatomedin
- Insulin-like growth factor 1
- Octreotide
At what time of the day does growth hormone secretion peak?
- During sleep
- During stress
- Postprandial
- Early in the morning
- During exercise
What is NOT stimulated by growth hormone?
- Decreased protein synthesis
- Lipolysis
- Sarcomere hypertrophy
- Gluconeogenesis
- Insulin-like growth factor 1 (IGF-1) secretion
In a patient who presents with a short stature, which symptoms are most suggestive of Frohlich syndrome?
- Hypogonadism, obesity
- Precocious puberty, obesity
- Precocious puberty, advanced bone age
- Hypogonadism, advanced bone age
- Normal puberty, advanced bone age
What is LEAST likely to trigger the release of growth hormone-releasing hormone?
- Feeding
- Sleep
- Exercise
- Hypoglycemia
- Stress
Author of lecture Control of Growth Hormone Release

Carlo Raj, MD
Customer reviews
2,5 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
The doctor speaks slowly, but covers the main components of the subject, explains their examples but is not as clear with common diseases as dwarfs.
Don't like the delivery very slow and need to play at 1.5 speed
