Playlist
Show Playlist
Hide Playlist
Cirrhosis with Case

-
Slides Gastroenterology 13 Liver Pt3 End Stage Liver Disease.pdf
-
Download Lecture Overview
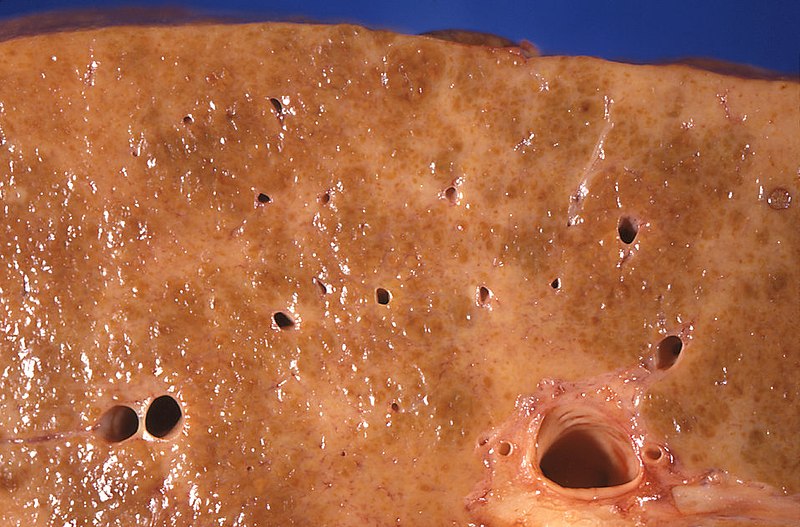
00:00 Welcome. 00:01 Today we'll discuss even further disorders of the liver and we'll specifically learn about end-stage liver disease. 00:08 So let's first begin by defining what is cirrhosis. 00:11 Eventually, with repetitive injury to the liver, you can develop advanced fibrosis leading to cirrhosis and ultimately, many of the downstream complications which include hepatocellular carcinoma. 00:27 So there are many common etiologies of cirrhosis. 00:30 The first category we can think about is inflammatory causes. 00:34 So this includes things like chronic viral hepatitis and autoimmune hepatitis among others. 00:41 Recall also that the liver is the place where we process many of the substances that we ingest, so any toxins can also lead to cirrhosis. 00:50 The most common of which is alcohol and medications that can be injurious to the liver. 00:57 Metabolic disease as we've also learned can contribute to cirrhosis in the case of non-alcoholic fatty liver disease. 01:04 And you may have congestion that leads to eventual scarring of the liver. 01:09 So things like congestive heart failure and veno-occlusive disease such as in Budd-Chiari syndrome. 01:16 You may also have congenital causes of cirrhosis, so this category includes alpha-1 antitrypsin deficiency, hemochromatosis and Wilson's disease. 01:25 And lastly, we have our last category of cryptogenic cirrhosis. 01:29 This is one we simply don't know the underlying cause and we just call it cryptogenic. 01:37 So now let's go to our cases. 01:39 Our first case is a 63-year-old man who presents to clinic with generalized pruritus for the last 3 months. 01:46 He notes yellowing of his eyes, fatigue and poor appetite for the same time period. 01:51 He has a history of hepatitis C for which he has never undergone treatment. 01:55 He has no sick contacts or recent travel. 01:58 His vitals are notable for a blood pressure of 95/53 mmHg. 02:02 His physical exam shows jaundice, palmar erythema and abdominal distention with a fluid wave. 02:10 Lab studies are notable for platelets of 55,000 (x10^9), INR 1.9 and serum albumin 2 (g/dL) with a bilirubin of 5.7 (mg/dL). 02:20 So what is the next step in confirming his diagnosis? Let's first go through some key items in this case. 02:28 So he has a nonspecific complaints of pruritus and yellowing of the eyes with fatigue that all localizes to the hepatobiliary system. 02:38 His history of hepatitis C is a known risk factor for cirrhosis. 02:43 And on exam, he has mild hypotension and physical exam findings of cirrhosis as we'll discuss later. 02:52 In addition, his labs are somewhat concerning for impaired liver synthetic function, which we'll also discuss. 03:00 So, let's first start with the clinical manifestations of cirrhosis. 03:04 We can break this down into the effects of portal hypertension, and effects from hepatocellular injury or liver cell failure. 03:16 So, we'll begin with the portal hypertension. 03:19 Due to high pressure in the portal systemic area, you may develop esophageal varices and gastropathy both of which can lead to GI bleeding as manifested by melena or hematemesis. 03:34 Patients may also develop splenomegaly which occurs after there's back up of flow into the splenic vessels. 03:43 Likewise, you may also have dilation of superficial blood vessels which then can lead to the typical appearance of caput medusae which are just dilated vessels on the superficial surface of the abdomen. 03:57 Patients may also develop ascites which is free fluid in the abdomen. 04:02 And they may have back up of flow into the rectal vessels leading to varices there which can manifest with hemorrhoids and lower GI bleeding. 04:12 On the other hand, if we talk about the effects of liver cell failure, patients may come in with confusion or coma from the build up of toxins. 04:22 They may also have skin findings of spider angiomata. 04:26 They may develop gynecomastia. 04:29 Both of these prior two things are due to imbalances of estrogen. 04:34 They may develop jaundice due to the build up of bilirubin. 04:38 They may develop asterixis which is also due to toxin build up. 04:44 They may have testicular atrophy, again related to the hormones. 04:48 They may have a risk of bleeding and they may develop ankle edema. 04:55 So now that we've gone through all the common symptoms or manifestations of cirrhosis, let's talk about what labs we often see. 05:02 So we can think about labs in 3 different categories: those that reflect the liver synthetic function, those that reflect hepatocellular injury and then a category of other labs that are affected. 05:14 So we will begin with the liver synthetic function. 05:17 These are the true things that reflect impaired synthesis within the liver: So low platelets or thrombocytopenia, you may have elevated prothrombin time or coagulopathy and you may have low albumin. 05:32 Now we move to the labs that reflect hepatocellular injury. 05:36 Patients may have elevated AST and ALT although note that this actually may be normal in certain cases. 05:43 They may also have a high alkaline phosphatase and they often have a high bilirubin. 05:49 Other labs that are often affected in cirrhosis include anemia, leukopenia - so low white cells, and low red cells, a reduced creatinine clearance and patients may develop hyponatremia from imbalances in free water. 06:05 So the diagnosis of cirrhosis is primarily an imaging diagnosis. 06:10 We use abdominal ultrasound as the test of choice because it is non-invasive and convenient. 06:17 There is a newer test called transient elastography that can be done to detect early fibrosis before patients have developed cirrhosis but this is beyond the scope of this lecture. 06:28 Liver biopsy is the gold standard for diagnosis but nowadays is usually not done because the diagnosis can be madeP with imaging. 06:37 So, some common ultrasound features as you can see here on the right are a nodular and coarse echotexture. 06:47 You may have reversal of portal flow which is not shown here but if you use Doppler with your ultrasound, you could then see this finding. 06:55 Patients may have splenomegaly or an enlarged spleen on ultrasound. 06:59 And shown here is the presence of ascites so that black-colored fluid above the surface of the liver is free fluid in the peritoneum, so ascites. 07:12 So now that we've gone through that, let's go back to our case. 07:16 Our 63-year-old man who's coming in with nonspecific complaints, some findings of jaundice. 07:22 He does have history of hepatitis C and he has physical exam findings now we know of cirrhosis. 07:28 In addition, he has impaired liver synthetic function on his labs with thrombocytopenia, an elevated INR and low albumin. 07:37 So what is the best next step in confirming his diagnosis? We now know the best test would be to do an abdominal ultrasound to confirm this diagnosis.
About the Lecture
The lecture Cirrhosis with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following is the initial diagnostic test of choice for cirrhosis?
- Abdominal ultrasonography
- Transient elastography
- Liver biopsy
- Abdominal CT
- Abdominal X-ray
Which of the following clinical manifestations of cirrhosis is caused by portal hypertension?
- Caput medusae
- Coma
- Jaundice
- Gynecomastia
- Somnolence
Which of the following clinical manifestations of cirrhosis is caused by liver cell failure?
- Coma
- Esophageal varices
- Caput medusae
- Hemorrhoids
- Ascites
Which of the following laboratory values reflects the decreased synthetic function of the liver?
- Elevated prothrombin time
- Elevated AST and ALT
- Elevated bilirubin
- Hyponatremia
- Anemia
Author of lecture Cirrhosis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
