Playlist
Show Playlist
Hide Playlist
Leukemia: Chronic Lymphoid Leukemia (CLL) – White Blood Cell Pathology

-
Slides Leukemia White Blood Cell Pathology.pdf
-
Download Lecture Overview
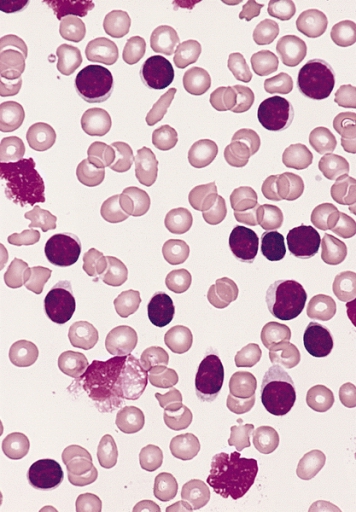
00:02 Let’s go into CLL. 00:05 This is chronic lymphocytic leukemia, and you see that this is then associated with SLL, small lymphoblastic or lymphocytic or lymphoma. 00:16 Why is CLL always associated with SLL, always? Diagnosis. 00:22 Basics. 00:23 Leukemia, the cancer began in the bone marrow, it then went into circulation, and then it got into your lymph node. 00:33 You could no longer call this CLL. 00:35 You will call this SLL. 00:37 From henceforth, you’ll never see a CLL without SLL. 00:39 They are partners for life. 00:41 Partners for life. 00:42 In fact, a very common cause of non-Hodgkin's lymphoma is CLL/SLL. 00:50 Think about what I just said. 00:52 Are you ever going to find Reed-Sternberg cell in a lymph node in a patient who’s 70-some years of age who has CLL/SLL? Are you going to find Reed-Sternberg cell? Of course not. 01:04 Maybe you find smudge cell or cracked chromatin, but you will never find a Reed-Sternberg cell. 01:09 If you don’t find a Reed-Sternberg cell and you have a lymphoma, you must call this a non-Hodgkin lymphoma. 01:17 So now, you have diffuse large B-cell lymphoma, you have follicular lymphoma, CLL/SLL, and multiple myeloma. 01:26 Eighty five percent of all of your non-Hodgkin’s lymphoma will be those four. 01:32 What are they? Diffuse large B-cell lymphoma, follicular lymphoma, this one, CLL/SLL, and multiple myeloma. 01:42 Are you getting smart about leukemias now, and lymphomas? Yeah, you are. 01:46 Now, neoplasm of maturing peripheral lymphocytes. 01:50 You only have two types, T-cells and B-cells. 01:52 Don’t ever forget this. 01:54 You’ll always find SLL attached to CLL. 01:58 They are partners for life. 02:00 The bone marrow is always involved, always. 02:02 That’s where the cancer originated from. 02:05 Spleen and liver can also be involved. 02:07 How old is your patient? Of all of the leukemias, all in general, this is the most common in the U.S. 02:14 So, this is the one you know -- you should know everything -- Actually, you know everything about every leukemia. 02:19 But particularly, this one, so this is by far the most common leukemia overall, older patient, older patient. 02:28 Now, specifically, the most common leukemia in young children will be ALL. 02:32 I’ll give you that, but overall, most common leukemia is this one, CLL/SLL. 02:37 Let’s continue. 02:38 CLL disrupts your normal immune function. 02:41 Why? Well, if you knock out your bone marrow and you don’t have proper B-cell production, how in the world are you going to then produce proper immunoglobulins? You cannot. 02:49 You have hypogammaglobulinemia, resulting in infections. 02:54 Also, big time, we talked about this hematology with RBC pathology. 02:59 And we looked at autoimmune hemolytic anemia, and I told you, I use a mnemonic. 03:04 It's cute. 03:05 I think warm in Georgia and cold in Michigan. 03:08 Warm type of autoimmune hemolytic anemia is IgG. 03:13 Could be associated, warm type of autoimmune hemolytic anemia. 03:17 Do not forget that. 03:19 Also, associated with immune thrombocytopenic purpura. 03:23 Immune thrombocytopenic purpura is when you have autoantibodies then attacking your glycoprotein IIb/IIIa, or maybe perhaps your glycoprotein Ib. 03:33 Important, important associations with CLL, you need to make sure you know all of these, please, before taking your boards and walking on through your wards. 03:43 Some CLLs will transform into a more aggressive form. 03:46 Stop here. 03:49 Blast crisis, is that what this is? Nope. 03:52 Okay, now open your eyes again. 03:54 CLL. 03:56 CML went to blast crisis. 03:59 When CML goes onto blast crisis, it may look like AML, but you will know enough information, you will know enough information to identify the proper leukemia. 04:10 CLL, if it goes onto aggressive form, if you remember correctly, and I know you do, that there are three ways in which you can then develop diffuse large B-cell lymphoma, three ways. 04:23 One was progression from follicular lymphoma. 04:27 Two was the fact, de novo, BCL6. 04:31 Oh yeah, this one. 04:33 CLL may go onto? Diffuse large B-cell lymphoma. 04:38 This is called Richter’s transformation. 04:40 Prolymphocytic transformation, known as a Richter, transformation into diffuse large B-cell lymphoma. 04:49 Third method of perhaps going onto diffuse large B-cell. 04:53 All? No, some. 04:58 With CLL, what are you going to find? Well, upon your morphology, you’ll find something called cracked chromatin, and you’ll find smudge cells as you see in the picture here. 05:08 You’re not going to find Reed-Sternberg. 05:11 Hence, if this enters a lymph node, what do you call this? Non-Hodgkin’s lymphoma. 05:17 Don’t forget that. 05:18 It is going to affect your lymph node, quite commonly, in these patients, so I keep bringing it up. 05:23 “Hey, doc” “Hey, doc” It’s just me impersonating being old. 05:28 “Hey, doc. I have a lump on my neck.” “Does it hurt?” “No, it doesn’t.” Okay, this is concerning. 05:34 You'd find cracked chromatin and smudge, CLL. 05:39 Clinically, your patient, median age of 60, oldest. 05:44 Take a look at the WBC count, 100,000. 05:48 Remember that topic that we had for extreme cases of neutrophilic leukocytosis, extreme cases? And at that time, I told you, what if the appendicitis ruptured or sepsis? Leukemoid reaction was what that was. 06:02 Here, we'd find WBC count greater than 100,000. 06:05 Insidious onset, once again. 06:07 Fatigue is going to be one of your common symptoms. 06:10 I told you earlier, please look for lymphadenopathy, and also hepatosplenomegaly. 06:16 Older patient. 06:18 Progression is slow but my goodness, if it transforms into what? The more aggressive form known as diffuse large B-cell lymphoma. 06:25 We have death within one year.
About the Lecture
The lecture Leukemia: Chronic Lymphoid Leukemia (CLL) – White Blood Cell Pathology by Carlo Raj, MD is from the course Leukemia – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following is least likely to be associated with chronic lymphoid leukemia?
- Polycythemia vera
- Hypogammaglobulinemia
- Autoimmune hemolytic anemia
- Immune thrombocytopenic purpura
- Small lymphocytic lymphoma
Into what kind of aggressive lymphoma is chronic lymphocytic leukemia most commonly transformed in Richter syndrome?
- Diffuse large b-cell lymphoma
- Chronic myeloid leukemia
- Acute myeloid leukemia
- Acute lymphoblastic leukemia
- Hairy cell leukemia
Which of the following cells are most often associated with chronic lymphocytic leukemia?
- Smudge cells
- Downey Cells
- Bite cells
- Popcorn cells
Author of lecture Leukemia: Chronic Lymphoid Leukemia (CLL) – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
