Playlist
Show Playlist
Hide Playlist
Carotid Stenosis: Etiology, Examination, Diagnosis

-
Slides CarotidStenosis Surgery V2.pdf
-
Download Lecture Overview
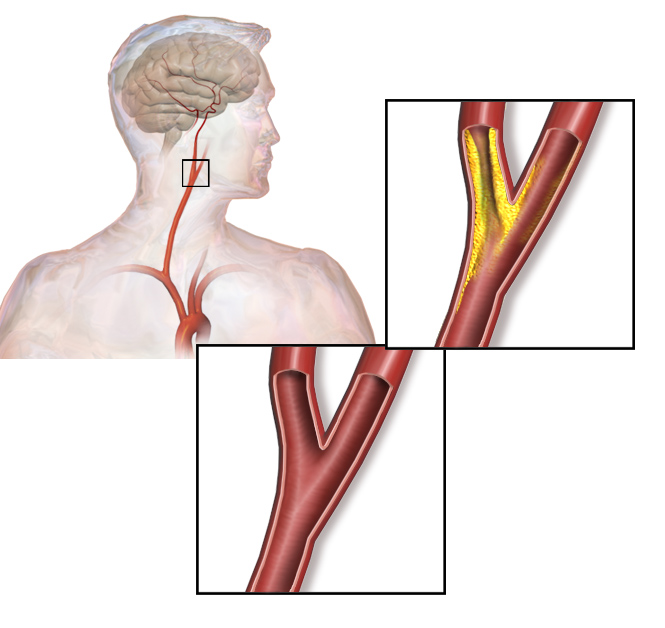
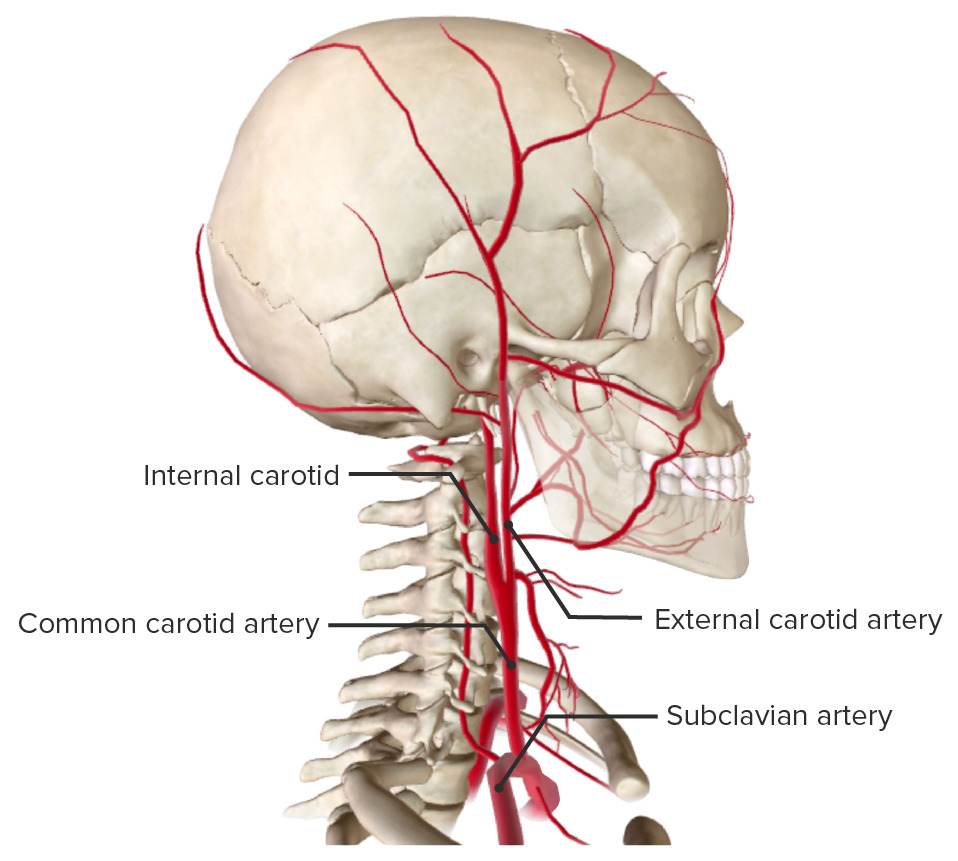
00:01 Welcome back. 00:02 Thanks for joining me on this discussion of carotid stenosis in the section of vascular surgery. 00:10 Carotid stenosis is a very common disease and there are some risk factors, particularly puts you at higher incidence. 00:17 For example, smoking. 00:19 In fact, smoking is a high-risk factor for most vascular diseases. 00:24 There is some association with increased alcohol intake and, of course, like any peripheral vascular disease, when one has one peripheral vascular disease, one is at a higher association for another. 00:38 In this situation, patients with coronary artery disease also may have carotid disease. 00:43 This is an important distinction, because when patients have coronary artery disease, also think about working them up for bilateral carotid diseases. 00:54 Let's discuss the pathophysiology of carotid diseases and atherosclerotic plaques. 01:01 Here's a depiction of a common carotid bifurcation. 01:05 It's, of course, situated in your neck. 01:06 You can feel your own carotid pulses. 01:09 Atherosclerotic plaques are dense in lipids and they usually occur at the carotid bifurcation. 01:17 This is particularly because, at the bifurcation, laminar or straight-line flow becomes turbulent. 01:24 And as turbulent flow occurs at the bifurcation, it perpetuates worsening of the atherosclerotic plaque. 01:32 At some point, the plaque becomes so thick that it actually narrows the lumen of the vessels. 01:38 That's when you become symptomatic. 01:43 What are some common findings of carotid stenosis? One might actually hear a carotid bruit. 01:48 When you listen to a patient who has a carotid stenosis, the carotid bruit actually sounds like, well, turbulent flow, as I previously described. 01:57 Some patients will also describe transient ischemic attacks, also known as TIAs. 02:04 In these select patients, it's a warning sign. 02:07 Patients may have intermittent stroke symptoms that are self-contained. 02:12 They may have completely resolved by the time the patient even presents to your office or the emergency room, but don't lose these patients to follow up. 02:21 They may actually have significant carotid disease. 02:27 This is a depiction of a curtain drawn down or a shade over a window. 02:32 And that's a classic description of amaurosis fugax. 02:36 That's the transient monocular blindness that's associated with plaques. 02:41 And those plaques may be distributing themselves into the ophthalmic artery. 02:45 Next. 02:46 Patients may actually have CVAs or stroke. 02:49 CVA stands for cerebrovascular accidents. 02:54 This is most likely due to portions of the atherosclerotic plaque breaking off and being embolic. 03:01 Also, when the channel is so stenotic that the flow is inadequate, one may actually have a broader distribution ischemic stroke. 03:10 Labs are unlikely to be helpful to you, but it is very important to screen for carotid disease when you have high suspicions. 03:18 How do we screen for carotid disease? I’ll give you a second to think about it. 03:25 That's right. 03:26 Carotid duplex ultrasonography. 03:29 As with all ultrasounds, the results and accuracy of these tests are heavily operator dependent. 03:35 Let's say the clinical scenario is a patient who presents to your office. 03:39 They describe symptoms consistent with TIAs or amaurosis fugax. 03:44 The next step of management will be obtain a carotid duplex ultrasound. 03:50 Duplexes are helpful not only because they give you anatomic information, but more importantly, for stenotic vessels, they give you velocity information. 04:00 Recall, flow through a smaller diameter is usually at higher velocities. 04:06 That’s simple physics. A certain velocity, as described as centimeters per second, is indicative of a percentage of carotid stenosis. 04:16 This is an approximation of course. 04:19 Angiography. 04:21 For many years, angiography was the gold standard. 04:24 I'm talking about the invasive interventional angiography, of course, not the spiral CAT scan angiographies. 04:32 In this representative invasive angiography, the arrow points at an area that’s most likely representative of a plaque. 04:39 Note, it's very close to the bifurcation.
About the Lecture
The lecture Carotid Stenosis: Etiology, Examination, Diagnosis by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
A patient presents with symptoms of amaurosis fugax. What is your first step in management?
- Obtain a carotid duplex ultrasound
- Perform carotid endarterectomy
- Obtain an echocardiogram
- Perform carotid stenting
- Perform applanation tonometry
Which of the following is NOT a risk factor for carotid stenosis?
- Marijuana abuse
- Smoking
- Coronary artery disease
- Alcohol
- High cholesterol levels
Author of lecture Carotid Stenosis: Etiology, Examination, Diagnosis

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Ecplained efficiently and accurately . Every thing is shown with good clariity and accuracy
