Playlist
Show Playlist
Hide Playlist
Cardiothoracic Surgery: Lung Cancer


-
Slides LungCancer Surgery.pdf
-
Download Lecture Overview
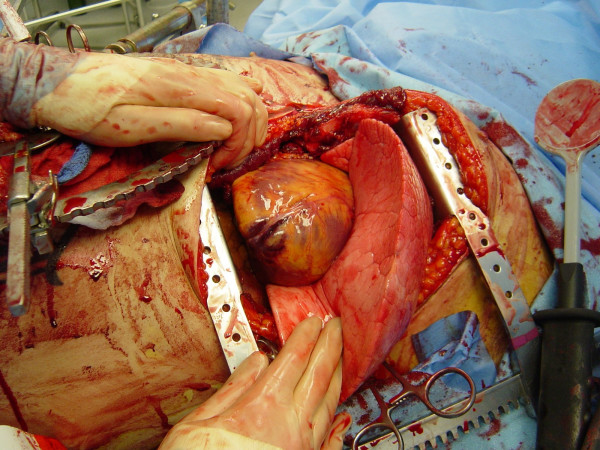
00:01 Thank you for joining me on this discussion of lung cancer in the section of cardiothoracic surgery. 00:09 Unfortunately, the incidence of lung cancer continues to rise. 00:14 And lung cancer is a malignancy of airways and lung parenchyma. 00:18 Smoking continues to be a pandemic across the world, which is why lung cancer continues to be one of the most common cancers. 00:26 Let's first discuss how we manage a solitary lung nodule. 00:31 A solitary lung nodule is defined as a discrete, well circumscribed lesion in the lung parenchyma. 00:39 Remember, these sometimes incidental findings are mostly benign. 00:43 So, don't alarm the patient too much prior to having biopsy results. 00:48 Remember, the anatomic location does not dictate whether the lesion is actually malignant or benign. 00:55 Let me ask you a question. 00:57 What makes the nodule then more likely to be malignant? I’ll give you a second to think about this. 01:04 That’s right. 01:05 The age of the patient, growth, and other risk factors, such as smoking, make a nodule more likely to be malignant. 01:13 Remember, the clinical scenario has to fit. 01:17 Here, you see a depiction of a pulmonary nodule in the left lower lobe. 01:22 Recall, there is a significant limitation to both cross-sectional imaging as well as routine x-rays. 01:28 Only lesions greater than 1 cm can be seen on a chest x-ray. 01:32 The good news is most lesions smaller than this are probably clinically insignificant. 01:38 So what happens if you find a solitary nodule on a chest x-ray? The correct thing to do is to try to find an older CXR to compare the size. 01:46 If it is same size, then it is benign and no further follow up is recommended. 01:50 If the nodule is growing then malignancy is likely and you should biopsy it. 01:54 If you have no older CXR or if it is equivocal, then you should get a CT. 01:59 The management mostly depends on the size of the nodule. 02:02 Now, how do we approach, once we've diagnosed lung cancer, the patient? Generally, lung cancer is divided into non-small cell lung cancer, mesothelioma, small cell lung cancer. 02:17 And under non-small cell lung cancer, specifically, there are two types - adenocarcinoma and squamous cell. 02:25 These have prognostic evaluation differences, although the treatment largely is the same. 02:31 Again, to remind you, lung cancer, the biggest risk factor is smoking and asbestos exposure. 02:40 Do you know what asbestos exposure is associated with? That's right. Mesothelioma. 02:48 Now, what specific physical findings might we encounter in somebody with lung cancer? If patients are actually symptomatic, it's important to remind you that it's usually late in the clinical presentation. 03:03 They may have chronic coughs, particularly hemoptysis. 03:07 Maybe they have post-obstructive pneumonia, pneumonia that develops as a result of an obstructing mass and the inability to clear secretions. 03:15 Bloody cough, pleuritic chest pain and dyspnea. 03:20 Again, all of these may be late signs of lung cancer. 03:23 And this slide demonstrates to you that hoarseness is also a late finding. 03:29 When a patient has lung cancer and develops hoarseness, it’s suggestive of a recurrent laryngeal nerve involvement. 03:37 Recall from our discussions of thyroid diseases, the recurrent laryngeal nerve can cause hoarseness or vocal paralysis. 03:45 Remember, if the recurrent laryngeal nerve is injured, the vocal cord actually goes into the resting medial position. 03:52 On cross-sectional imaging, or a CAT scan of the chest, you may notice a pleural effusion. 03:58 Pleural effusion signifies pleural involvement. 04:02 Remember, not all pleural effusions in patients with nodules are malignant in nature. 04:07 If you were to tap this fluid, you would most likely note that it includes oncologic cells as well as blood. 04:14 That's called a malignant effusion. 04:17 Now, let's discuss a favorite topic of examinations. 04:23 The superior vena cava syndrome. 04:25 Superior vena cava syndrome results in dilated neck veins due to poor superior vena cava drainage. 04:32 Sometimes, there's plethora of the face due to facial edema, again, due to the lack of venous return. 04:38 And it's typically associated with right hilar masses that obstruct the SVC or superior vena cava drainage. 04:45 Now, what about a Pancoast tumor? It's important for you to remember the Horner syndrome. 04:51 Horner syndrome is a constellation of symptoms including meiosis and ptosis, dropping of the eyelids, sometimes shoulder pain, atrophy of the hand muscles on the affected side, and sometimes bony destruction. 05:09 Horner syndrome is a constellation of symptoms described as ocular sympathetic paresis. 05:14 This is due to a lesion invading the sympathetic chain. 05:17 Again, to remind you, meiosis, ptosis and anhidrosis, this is a classic association. 05:25 When presented with this clinical syndrome on your examination, remember Horner syndrome. 05:30 Now, let's visit another favorite topic called paraneoplastic syndromes. 05:35 Remember, up to 10% of patients with lung cancer may have an associated paraneoplastic syndrome, most commonly symptom of inappropriate antidiuretic hormone. 05:45 Remember, these are extra organ associated secretions and do not subject themselves to feedback mechanisms. 05:54 This can relate to humoral hypercalcemia in patients who have parathyroid like hormone secretions. 06:01 SIADH secretion is usually associated with small cell lung cancer. 06:07 Remember that association. 06:08 And can lead to significant hyponatremia. 06:12 SIADH induces increased antidiuretic hormone retention. 06:17 As a result, significant volume retention occurs. 06:22 Now, let's talk about the mechanism behind humoral hypercalcemia and other paraneoplastic syndrome. 06:28 This is related to parathyroid-related protein (PTHRP). 06:33 As a result of parathyroid-related protein secretions, there may be signs of increased tumor burden and signal late disease burden. 06:41 Symptoms are similar to other signs of hypercalcemia. 06:45 It's worthwhile to remember, patients may have groans, moans and psychiatric overtones. 06:51 Now, what about cortisol? An ectopic Cushing syndrome is also a potential paraneoplastic syndrome. 06:57 Hypercortisolism results in uncontrolled ACTH, again, associated with small cell lung cancer. 07:06 Patients demonstrate, as anybody with high cortisol levels, including moon faces, acne, purple striae, muscle weakness, edema and alkalosis with hypokalemia. 07:21 Now, unfortunately, no significant routine laboratory values will indicate a diagnosis of lung cancer. 07:30 We’ve discussed CT scans. Note, left lower lobe a nodule. 07:35 This may be suggestive of lung cancer. 07:38 Oftentimes, patients suspected of lung cancer or biopsy proven have obtained a PET scan. 07:44 Remember, cancer processes are more PET-avid. 07:49 In this image, you see a right upper lobe lesion, suspicious. 07:53 Now, let’s talk about biopsies. 07:55 Biopsies can be obtained through several, depending on the location of the tumor. 08:00 Bronchoscopic biopsies with ultrasound guidance is becoming more and more of a standard. 08:05 It can be done in a sedated patient on an outpatient basis. 08:09 If your sample is inadequate, you may require surgical sampling. 08:14 Sometimes with surgical sampling, the entire lesion is removed. 08:18 That’s called an excisional biopsy. 08:20 Let’s discuss non-small cell lung cancers. 08:23 Determination of the resectability or their lack of metastases is the single most important decision before moving or offering surgery. 08:33 For early stage cancers, the treatment options include resection and adjuvant therapy. 08:39 However, for late stage cancers, start with neoadjuvant therapy and reassess whether or not the tumor is resectable. 08:47 Remember, when offering resection to a patient, curative intent is the purpose. 08:54 Functional status is an important determinant, whether the patient can undergo surgery. 08:58 Not only their risk of having a heart attack around the surgery, but also what is their residual lung function. 09:05 Now, let's move on to small cell lung cancer. 09:08 In these set of images, ones notes the right lower lobe lesion, highlighted by the green. 09:13 Small cell lung cancers are a little bit different. 09:16 They’re usually chemo responsive. 09:18 Unfortunately, they’re usually disseminated at the presentation. 09:22 So, surgery for these patients is quite rare. 09:25 Here's an image of surgery for lung cancer. 09:28 Depending on the size and the modality, these surgeries can be done in an open or, in this scenario, a VAS or video assisted surgery. 09:37 Here, in the right lower quadrant of the four series, you notice a stapler coming across hilar vessels. 09:44 Now, it is time to review some important clinical pearls and high-yield information. 09:49 Remember, you should undertake an extensive metastatic workup prior to offering resection. 09:55 And if a patient has a malignant effusion, it's considered advanced disease. 10:00 Remember a favorite of USMLE exam questions is Horner syndrome. 10:05 Horner syndrome is a constellation of meiosis, ptosis and anhidrosis. 10:11 Thank you very much for joining me on this discussion of lung cancers.
About the Lecture
The lecture Cardiothoracic Surgery: Lung Cancer by Kevin Pei, MD is from the course Special Surgery. It contains the following chapters:
- Cardiothoracic Surgery – Lung Cancer
- Paraneoplastic Syndromes
- NSCLC and SCLC
Included Quiz Questions
Which of the following types of cancers is the most common non-small cell lung cancer?
- Adenocarcinoma
- Mesothelioma
- Hypopharyngeal Cancer
- Carcinoid tumor
- Lymphoma
Which of the following findings are NOT present in superior vena cava syndrome?
- Pleuritic chest pain
- Dilated neck veins
- Right hilar mass
- Plethoric appearance
- Facial edema
Horner syndrome is a constellation of which of the following findings?
- Miosis, ptosis, and anhidrosis
- Miosis, hyperhidrosis, and ptosis
- Hyperhidrosis, mydriasis, and ptosis
- Ptosis, mydriasis, and eye twitching
- Anhidrosis, mydriasis, and ptosis
Which of the following findings is NOT seen in ectopic Cushing’s syndrome?
- Hyperkalemia
- Purple striae
- Edema
- Muscle weakness
- Acne
Elevations of what lab value is commonly associated with malignancy-associated hypercalcemia?
- PTHrP
- BDNF
- MHC
- 1,25-(OH)₂D
- BCGF
Author of lecture Cardiothoracic Surgery: Lung Cancer

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
