Playlist
Show Playlist
Hide Playlist
Cardiac Case: 45-year-old Man with Alcohol Intake after Minor Traffic Accident

-
Cardiac Case 45-year-old Man with Alcohol Intake after Minor Traffic Accident.pdf
-
Download Lecture Overview
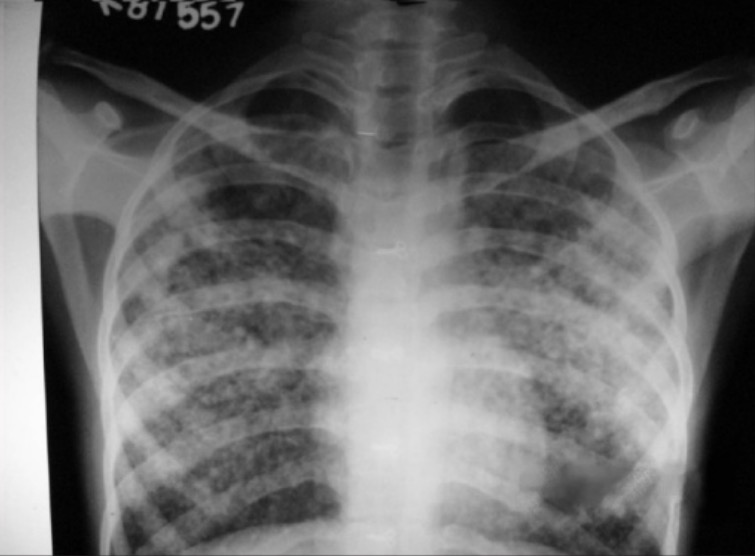
00:01 a 45-year-old man is brought to the emergency department following a minor traffic accident. 00:06 At the scene of the accident, the police noted that he smelled of alcohol and was confused. 00:12 He has consumed one liter of vodka per day for 20 years. 00:16 On physical exam, the blood pressure's elevated at 155/90 mmHg as is the heart rate at a 102/min, jugular venous pulse is also elevated 15 cm of water demonstrating that right atrial pressure is elevated. 00:29 The respiratory sounds on the lung exam showed diffused wheezes and crackles and there's a prominent third heart sound. 00:36 That's the sound of heart failure marked decrease compliance or elasticity in the left ventricle and let's have a demonstration. 00:45 Here's a normal heart, lub-dub, lub-dub, lub-dub. 00:50 Here's the third heart sound, lub-dubd, lub-dubd, lub-dubd, and the abdomen is distended, the liver's not palpable, probably shrunken by cirrhosis, the distended abdomen is probably ascites, that is fluid in the abdomen in end-stage liver disease. 01:05 And he has 3+ pitting edema again, a sign of heart failure. 01:09 On laboratory he's anemic with a low white blood cell count and low platelet count quite common in end-stage liver disease. 01:16 Fortunately, his kidneys are still working well. His creatinine is normal. 01:19 And the liver function test demonstrates, of course marked abnormality. 01:23 His bilirubin is 12 mg/dL. His brain natriuretic peptide or BNP is elevated at 2000 pg/mL implying significant volume overload. 01:33 Just to go through the critical points in the story, he's an alcoholic with a huge alcohol consumption for many years. 01:41 His blood pressure's elevated, not uncommon in alcoholics. 01:45 Heart rate also along with the jugular venous pulse and the crackles in the lung and the third heart sound tell you that there's left ventricular failure. 01:54 His abdomen is distended implying that he has ascites that is fluid in the abdomen a sign of end-stage liver disease and of course, his extremities head edema also part of the heart failure. 02:06 He's anemic, has a low white blood cell count and a low platelet count all of which go with end-stage liver disease and of course, his liver function tests are very abnormal and his brain natriuretic peptide or BNP test is telling us that there's heart failure. 02:22 Here's his chest X-ray. It' clear he's in pulmonary edema. 02:26 There's lots of excess fluid in the lung and the heart appears large although on a PNS X-ray you can't be a hundred percent certain. 02:34 The first diagnostic test is an echocardiogram which confirms that this man has severe damage to his left ventricle. 02:40 The left ventricular ejection fraction is only 15%, normal would be above 50% and he has a variety of blood tests and ultrasound showing that he has advanced cirrhosis of the liver and his physical exam suggests also ascites secondary to portal hypertension. 02:59 So, the diagnosis: pulmonary edema secondary to alcohol induced cardiomyopathy. 03:06 Alcohol intake in large amounts is a toxin to the myocardium and taken over many years results in very severe myocardial damage to the left ventricle. 03:17 If the patient stops drinking soon enough, there can be recovery but if it's been going on for a very long time, there may be no recovery. 03:24 Well, to make the patient more comfortable, we give intravenous diuretics to induce a diuresis to get rid of some of the excess alcohol. 03:33 We have to have alcohol withdrawal monitoring to make sure the patient doesn't go into delirium tremens and there's a whole protocol for that, the so-called 'CIWA protocol'. 03:42 And then he needs a heart failure evaluation and management probably since his creatinine is normal, we would use ACE inhibitors that is angiotensin converting enzyme inhibitors or angiotensin receptor blockers as well as a trial for beta blockers such as carvedilol. 03:59 And it would be important for him absolutely not to drink ever again. 04:03 I tell patients like this, 'for you alcohol is poison'. 04:07 So in follow up, he diuresis, he loses 32 lbs over a couple of weeks. 04:14 He starts on low doses of carvedilol, lisinopril as an angiotensin converting enzyme inhibitor, spironolactone blocks aldosterone also part of the renin angiotensin system and we start with low doses in his medicines and gradually increased. 04:31 For patients such as this one with heart failure with reduced ejection fraction, of course referred to as HfRef, as we talk about. 04:39 If patients have contraindications to any of the renin angiotensin system antagonists, an alternative is hydralazine plus a long-acting nitrate. 04:48 In patients who still have symptomatic heart failure, secondary therapies may be added in addition to the initial medications. 04:56 These include mineralocorticoid receptor antagonists such as spironolactone that I just mentioned, or SGLT2 Inhibitors. 05:05 If further secondary therapies are needed, newer medications include verciquat or ivabradine. 05:13 and as we talkt about befor Vericiguat is indicated for people with New York heart association class 2 to 4 heart failure with an ejection fraction less than 45% who were either hospitalized in the last 6 months or required outpatient IV diuretics. 05:30 Ivabradine is a newer class of medication called a hyperpolarization-activated cyclic nucleotide-gated (HCN) channel blocker It is indicated for patients with an ejection fraction 35% or less who are in sinus rhythm with a resting heart rate at least 70 beats a minute or more despite beta blockers or with contraindications to beta blockers or contra indications to beta blockers. 05:55 Ivabradine works by slowing the sinus node by slowing the spontaneous ingress of sodium through the so-called funny channel into the sinus node cells. 06:08 He has a coronary angiogram to make sure he doesn't have coronary disease. 06:11 It's normal which is quite common in alcoholics since cholesterol is produced in the liver. 06:16 And when you have a liver that's not working, usually the cholesterol's quite low. 06:20 The abdominal ultrasound confirms liver cirrhosis and ascites and of course, we recommend that he never drink alcohol again.
About the Lecture
The lecture Cardiac Case: 45-year-old Man with Alcohol Intake after Minor Traffic Accident by Joseph Alpert, MD is from the course Cardiovascular Cases.
Included Quiz Questions
Which of the following is true of the third heart sound noted in this patient?
- It is a sign of decreased compliance.
- It is the sound of the mitral or tricuspid valve closing.
- It is the sound of the aortic and pulmonary valves closing.
- It is a sign of high atrial pressure.
- It is a sign of reduced ventricular filling.
An elevated brain natriuretic peptide (BNP) level most likely indicates which of the following?
- Worsening heart failure
- Systemic hypotension
- Tamponade
- Liver damage
- Inflammation
Author of lecture Cardiac Case: 45-year-old Man with Alcohol Intake after Minor Traffic Accident

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
