Playlist
Show Playlist
Hide Playlist
Bundle Branch and Fascicular Blocks

-
Slides Bundle Branch and Fascicular Blocks.pdf
-
Download Lecture Overview
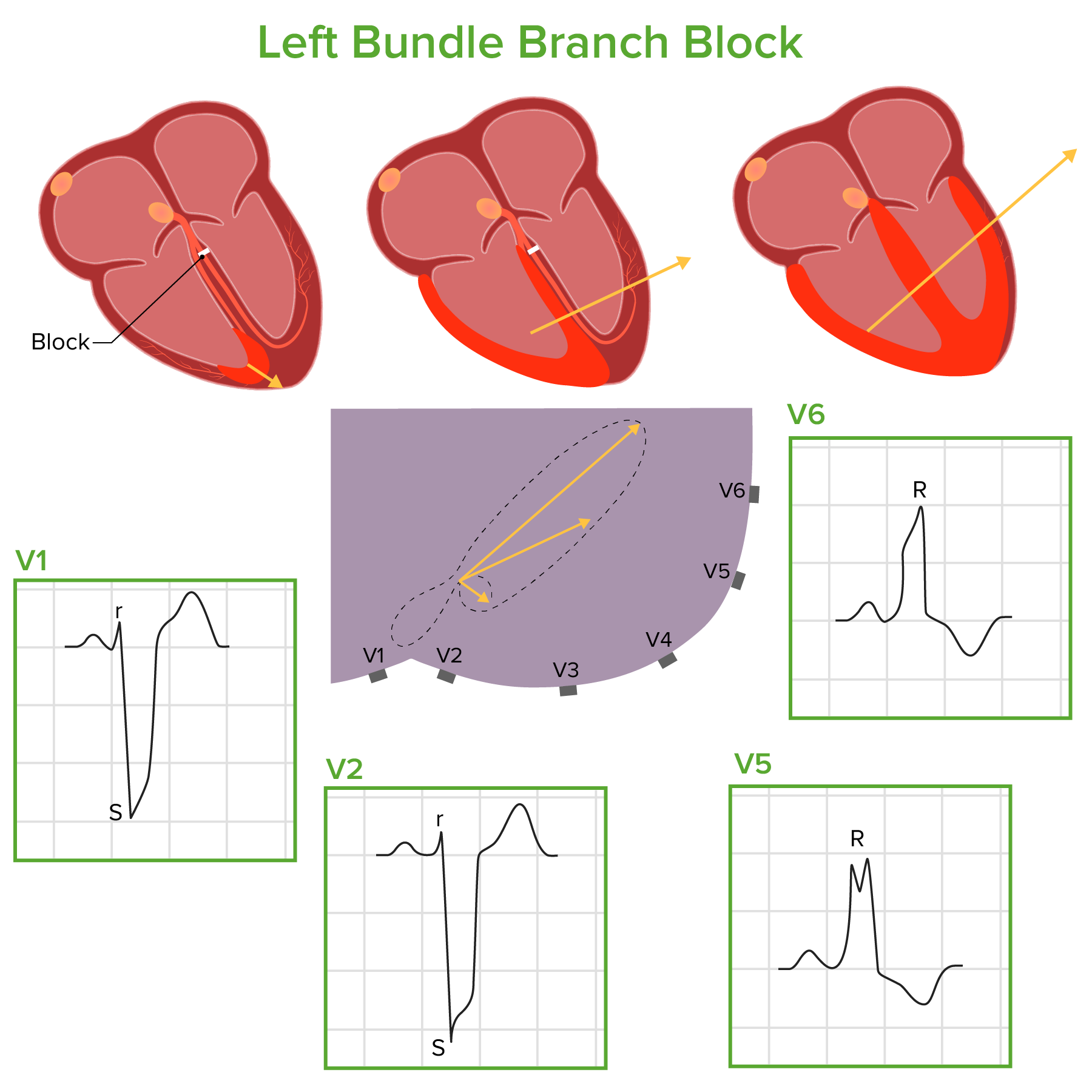
00:01 And the membrane resets during the T wave phase and is ready for the next electrical wave. 00:07 And so when there are damages to the elements of the conduction system, they delay atrial or ventricular contraction and these damage to the elements of the conduction system can lead to either sick sinus syndrome, abnormality in the sinus node or it can lead to abnormalities in the ventricular system which is seen as bundle branch block. 00:30 Let's look first at the damage sinus node. 00:33 A failure of the node to start the electrical wave markedly slows the heart rate or causes a delayed heartbeat. 00:41 And abnormal sinus node function is quite common in elderly patients and it’s called sick sinus syndrome. 00:48 And it's often associated with periods of very slow heart rate followed by arrhythmias where the heart rate's very fast and is often treated with pacemaker and we're gonna talk about that later when we talk about arrhythmias. 01:00 What about the bundle branch block? Abnormalities in the right or left bundle branches lead to a widened QRS so greater than 0.10. 01:09 And a QRS of 0.11 is sort of a nonspecific conduction delay. 01:15 But when it's 0.12 or more, it's called a bundle branch block, either right or left. 01:21 So let's look first at right bundle branch block. 01:25 Here is the typical right bundle branch block pattern. First of all, deep S wave in lead V1. Why? Because there's late depolarization of the right ventricle and parts of the septum that are supplied by the right bundle. 01:42 And there's also deep S waves in V6. 01:44 Again showing late slow depolarization in the areas of the right bundle. 01:52 In addition, there's the famous so-called rabbit ears. 01:55 In lead V1, there's two upward deflections. 02:00 In other words there's an R and an S and then the so-called R prime or a second R, so-called rabbit ears. 02:08 And the rabbit ears can be a different size. 02:10 I'll show you an example where there was a little tiny initial rabbit ear and a big second one. 02:15 You - and I'll show you an example where both rabbit ears are of equal size. 02:19 Notice again in V1 the deep S waves, notice also, look down in V6, there are deep S waves. 02:25 So this is a right - and the right bundle is reflected in a QRS duration of 0.14 seconds, greater than 0.12, so this is a typical right bundle branch block. 02:37 Here's another right bundle branch block. Notice the rabbit ears. 02:42 Notice that the first rabbit ear in lead V1 is pretty small and even in V2. 02:47 And there's a - the second rabbit ear is quite big. 02:50 But again the duration of the QRS is 0.14 seconds. 02:56 And you'll notice also a big broad S wave in lead V6. See the rabbit ears and the deep S wave in V6. 03:06 And here, the QRS duration is even longer than 0.14, it's 0.16. 03:13 Here's another - this is a more typical example of rabbit ears. 03:17 You see both rabbit ears are about the same size. It's a wide QRS. 03:22 Notice there's also in lead V6 and lead I a wide S wave. 03:28 Here, the rabbit ears are much more typical and the QRS duration here is 0.14 seconds. 03:35 And here's another example of a bundle branch block. Is this the right bundle or not? Look at it for a moment and think about it. 03:51 Do you see rabbit ears? I don't see any rabbit ears. 03:54 In fact what you see, a wide QRS, 0.14 seconds, big upright R wave in lead I and a big broad upright R wave in lead V6 and broad S waves in lead V1, V2, V3. 04:13 So this is an example of left bundle branch block. 04:17 Wide QRS in all the leads, again the upright broad pattern in lead 1 and V6. 04:27 And there's often ST abnormalities. Mark ST elevation. 04:32 So this EKG is sometimes mistaken for an acute MI, but you gotta look at the width of the QRS. 04:38 If it's greater than 0.12, it's a left bundle and you can't read a myocardial infarct with a left bundle branch block. 04:46 Now, here's one where the QRS duration is only 0.11. So it's a little bit left bundle-ish, right? Look at lead I and lead V6. 04:56 There's no rabbit ears, so often, this is called a nonspecific ventricular conduction delay. 05:03 So there's a block in part of the left bundle but it really isn't enough to be called a left bundle or a right bundle. 05:12 Now you can see blocks in part of the left to right bundle - left bundle rather. 05:18 You can see blocks in the anterior portion of the left bundle or in the posterior. 05:22 Let's look at these. Let's look at the first one, there's the block in the anterior portion of the left bundle, sometimes called left anterior hemi block or half block or the left anterior fascicular block. 05:38 First thing you see when you knock out the left anterior half of the left bundle is there's a marked axis deviation to more than 45 degree. 05:50 So -45 or -60, so up this direction, you see a small Q wave in aVL. 05:59 And it can't be diagnosed when there's an inferior wall myocardial infarction cuz that often results in a marked left axis. 06:07 So that takes away the criteria for a left anterior hemi block. 06:12 Left anterior hemi block is quite common and it doesn't imply serious heart disease. 06:19 It's only a little bit of the left bundle that's a blocked. Here's a typical example. 06:25 You can see marked left axis deviation, notice that the tallest R wave here is in lead aVL so that the left axis is -60. There's a widened QRS generally 0.11, something like that. 06:41 And there's a small Q in lead aVL. So left anterior hemi block. 06:46 Block in the posterior portion of the left bundle is more serious. Why? The left anterior branch is very small and thin and it can easily be damaged by scarring or hypertrophy of the ventricles and so forth as people age. 07:03 The left posterior bundle is huge and broad so when it's damaged leading to left posterior hemi block, it usually means there's a lot of injury to the ventricle. 07:13 So, let's look at it - the posterior hemi block characteristics. 07:18 Notice first of all the frontal plane axis goes in the opposite direction, right? Remember left anterior hemi block was -60 - 45 to 60. 07:28 But left posterior hemi block is +90 to 180 and the QRS is still not more than 0.12 cuz if it was more than 0.12 it will be left - full left bundle branch block. 07:41 It's uncommon due to the broad nature of the posterior bundle as I said. 07:45 And it also has a dual blood supply so it usually survives even when the left anterior bundle is knocked out. 07:53 And here we see an example, notice leads - in the green box, leads III and AVF are the maximum R wave. 08:01 Remember lead III is +120, lead AVF is +90 so it's somewhere between 90 and 120. 08:08 So in this case, the computer has calculated it as +100. 08:12 And you'll notice that the QRS is not wide enough to be a left bundle branch block. 08:19 So left anterior fascicular block is common not due to severe damage to the conduction system. 08:27 Left posterior fascicular block, uncommon and due to important damage to the conduction system. 08:33 Left bundle branch block almost always occurs in association with one or another form of serious heart disease for example; cardiomyopathy. 08:41 So left anterior fascicular block can be just an aging change. 08:46 Left posterior and left bundle usually imply more serious heart disease for example previous myocardial infarction or cardiomyopathy.
About the Lecture
The lecture Bundle Branch and Fascicular Blocks by Joseph Alpert, MD is from the course Electrocardiogram (ECG) Interpretation. It contains the following chapters:
- Bundle Branch Blocks
- Right Bundle Branch Block
- Left Bundle Branch Block
- Left Anterior Hemiblock
- Left Posterior Hemiblock
Included Quiz Questions
Which of the following is associated with sick sinus syndrome?
- Treatment with a pacemaker
- A very fast heart rate followed by arrhythmias
- Blockage in the His-Purkinje system
- Young patients
Which of the following is diagnostic of a right bundle branch block?
- QRS duration of > 0.12 seconds, deep S waves in leads I and V6, and presence of 'rabbit ears' in V1–V2
- Tall R waves in V1, deep S waves in aVL, and tall P waves in V3
- High voltages in leads V4, V5, and V6 as well as a prominent R wave in V1
- Left-axis deviation to –60 °, widened QRS, and small Q in lead aVL
- Wide QRS, large R wave in leads I and V6, and broad S waves in V1–V3
Which set of findings is diagnostic for a left bundle branch block?
- QRS duration of > 0.12 seconds, large R wave in leads I and V6, and broad S waves in V1–V3
- Tall R waves in V1, deep S waves in aVL, and tall P waves in V3
- High voltages in leads V4, V5, and V6 as well as a prominent R wave in V1
- Left axis deviation to –60°, widened QRS, and small Q in lead aVL
- QRS duration of > 0.10 seconds, deep S waves in leads V1 and V6, and presence of 'rabbit ears' in V1–V2
Which of the following is most characteristic of a left anterior fascicular block (LAFB), or left anterior hemiblock?
- Abnormal left axis deviation, QRS duration of 0.11 sec, and small Q in lead aVL
- QRS duration of > 0.10 seconds, large R wave in leads I and V6, and broad S waves in V1–V3
- Tall R waves in V1, deep S waves in aVL, and tall P waves in V3
- High voltages in leads V4, V5, and V6 as well as a prominent R wave in V1
- QRS duration of >0.10 seconds, deep S waves in leads V1 and V6, and presence of 'rabbit ears' in V1–V2
Author of lecture Bundle Branch and Fascicular Blocks

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
