Playlist
Show Playlist
Hide Playlist
Breastfeeding Problems

-
Slides NewbornAnticipatoryGuidance Pediatrics.pdf
-
Download Lecture Overview
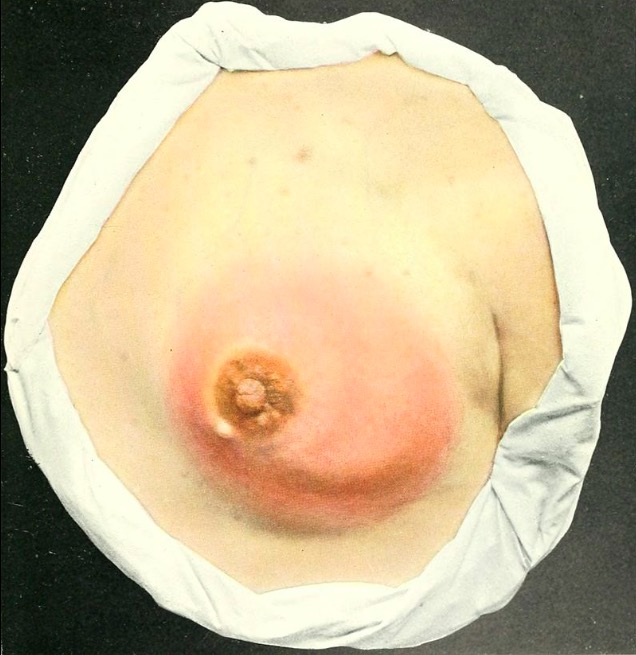
00:01 So there are many breastfeeding problems that occur to parents, especially new mothers who don't know what they're doing. 00:07 The first is sore nipples. That's common, very common. 00:13 The first thing we want to do is make sure the latch is good. 00:16 Make sure that baby's mouth is wide open when it accepts the breast. 00:20 So inspect that latch and make sure it's good. 00:23 Make sure the tongue is positioned appropriately. 00:26 We should provide therapy for sore nipples as well. 00:29 So for example, what we will often do is do cold packs after breastfeeding and may be even warm packs before breastfeeding to help engorge the breast. 00:39 So breast engorgement when it's too full is often a result of inadequate frequency of breastfeeding. 00:47 The mother should be encouraged to feed more often. 00:50 Also, it can be from ineffective feeding. 00:54 That's also a problem. 00:55 Sometimes it's because mothers are always starting on one side but not the other. 01:00 So we should encourage mothers to alternate which side they start the baby on. 01:05 Remember that baby's going to eat for may be 5-10 minutes and then switch breast to the other side. 01:09 The second breast, the baby is may be a little bit less vigorous and breasts only make as much milk as they are demanded off. 01:15 So if they always start on one side, gradually one breast will grow bigger than the other. 01:21 The other one is plugged ducts. 01:22 So if you warm it before and cold it after, that will help. 01:26 Also varied positions help and it's important to know what are the breastfeeding positions, so you can teach that to the parent. 01:33 Here is the cross-cradle position or they could use the supine position. 01:38 Or they can use the football hold position. 01:41 Any of these are fine, in terms of allowing the baby to breastfeed. 01:45 And sometimes, varying positions allow the baby to suck at the breast from different angles which allows those ducts to empty out. 01:52 Next is mastitis. This can sometimes come up. 01:57 Any pregnant or breastfeeding mother should know that after she has been breastfeeding for a while, if she develops fever and has no other symptoms, she should be seen for potential mastitis. 02:07 After a while, after that fever is out, often they'll get redness over the breast and rarely there can be an abscess. 02:14 So the redness may be delayed, but you should continue to feed through a breast that is infected because that will actually make her get better faster. 02:23 It will help unplug those ducts. And we will provide antibiotics, but those are antibiotics that are safe for the baby to get in a breast milk. 02:31 Another complication is jaundice. There are two types of jaundice. 02:36 This is a common test question. The first is breastfeeding jaundice. 02:41 That's when a baby is not eating enough. 02:44 We call it breastfeeding jaundice because of that colostrum. 02:47 They are not generating enough stools. 02:50 Remember, stool is how we get the jaundice out of the baby through the biliary tract. 02:55 Another type of jaundice that's specific to breastfeeding is breast milk jaundice. 03:01 This typically happens around the age of 10-14 days and it is a transient phenomenon and you should feed through it. 03:10 In very extreme cases, you might bottle feed for a day and let mom pump, and then go back to breastfeeding. 03:16 But you should not stop breast expression because of breast milk jaundice. 03:20 What's happening is there some undefined factor in breast milk that actually reduces the conversion of bilirubin in the liver and extrusion of bilirubin out into the biliary tree. 03:32 Nobody knows why it happens, but it's well-described. 03:35 It does not happen with formula, but it's transient and benign. 03:39 Okay. Formula feeding. 03:41 Let's say I'm on the side she doesn't want to breastfeed or she hasn't breastfed before or for whatever reason, she's chosen to use formula. 03:49 That's fine. There are generally many different type of formula which she can choose from and formula companies will market themselves to parents. 03:59 We should avoid letting mothers get confused by this marketing. 04:04 A lot of the marketing is flat out wrong. 04:07 So, what should she choose? Well, the first line agent is usually a milk-based formula. 04:14 She may say something like, "I was allergic to milk-based formula, when I was a kid so I want to start soy." It's probably not worth getting in an argument about if somebody feels very passionately to start soymilk but it's probably not necessary. 04:29 Remember, propensity for allergy is inherited, but what that allergy is, is not inherited. 04:35 So that baby most likely will tolerate cow's milk-based formula just fine, but if they don't want that, they can certainly choose a soy-based formula. 04:45 There is no real benefit here, this is really personal choice. 04:49 However, there are special formulas for patients who have true milk protein allergy. 04:55 If your baby has blood in the stool or gets very sick with blood in the stool, your baby may have a milk protein allergy. 05:03 Very rarely, it can be from fussiness, but most infantile fussiness is not a formula issue, it's an issue with colic. 05:12 That aside, we have this special hydrolyzed formulas for this purpose like Nutramigen or Alimentum. 05:18 It's important that if a child is on milk-based formula and they have a true allergic response, they should not be placed on soy formula. 05:27 Let me say that again, they should not be placed on soy formula. 05:31 They should go straight to an alimental formula. 05:34 The reason for that is there's a lot of cross-allergy between these two formulas, so infants on milk who have allergy may still have the allergy on the soy formula and some of those kids can get quite sick.
About the Lecture
The lecture Breastfeeding Problems by Brian Alverson, MD is from the course Neonatology (Newborn Medicine).
Included Quiz Questions
Which of the following is NOT a common breastfeeding problem?
- Disinterest of the baby in feeding
- Sore nipples
- Engorgement of the breast prior to feeding
- Plugged ducts
- Neonatal jaundice
Breast engorgement in a nursing mother is most likely to occur due to which of the following?
- Inadequate frequency of breastfeeding
- Maternal malnutrition
- Sore nipples
- Young maternal age
- Maternal age over 30
Breast milk jaundice occurs at which age?
- 10–14 days
- 2–3 days
- Day 1
- 4–8 days
- > 21 days
Which of the following is the most appropriate type of formula for patients with established allergy to cow milk protein-based formula?
- Protein hydrolysate formula
- Soy-based formula
- Concentrated liquid formula
- Powdered formula
Author of lecture Breastfeeding Problems

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
The essential information, well structured and presented. It will help me with the parents to provide better advice.
